Murro Rachel, El Ayadi Alison M, Patil Rutuja, Agarwal Dhiraj, Juvekar Sanjay, Kim Juliana, Diamond-Smith Nadia G
Department of Epidemiology and Biostatistics, University of California, San Francisco, 550 16th St 2nd Floor, San Francisco CA 94158 USA.
Department of Obstetrics, Gynecology, & Reproductive Sciences, University of California, San Francisco, 550 16th Street, #3745, San Francisco CA 94158 USA.
J Migr Health. 2025 Mar 29;11:100322. doi: 10.1016/j.jmh.2025.100322. eCollection 2025.
Maternal health in rural India has improved due to national initiatives, but inadequate healthcare provision persists across most sociodemographic groups. The connection between perinatal care and the widespread practice of Temporary Childbirth Migration (TCM)-returning to one's natal home for delivery and the postpartum period-remains unexplored.
Cross-sectional data on migration and health visits were collected from a sample of 1288 women in the Vadu Health and Demographic Surveillance Site (HDSS) (Western Maharashtra) who gave birth in 2018-2022. Childbirth migration (exposure) was analyzed in three ways: binary (any migration), continuous (duration of stay), and multidimensional (duration of stay and change of provider). Outcomes included number of health visits - both facility check-ups and home visits by community health workers - and early antenatal care initiation. Multivariate poisson, negative binomial and logistic regressions were used. Sensitivity analyses checked for recall bias, the influence of migration distance, and model misspecification.
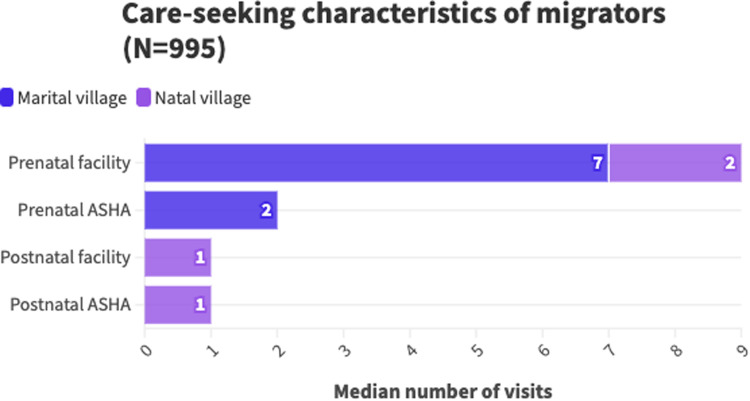
Migrators and non-migrators had similar outcomes in early antenatal care initiation, facility visits (before and after pregnancy), and prenatal community health worker visits. Migrators had fewer postnatal community health worker visits (IRR = 0.80; 95 % CI 0.70-0.92). Among migrators, longer natal village stays were associated with fewer community health worker visits in the prenatal period (IRR = 0.92; 95 % CI 0.88-0.96) but not postnatally (IRR = 1.03; 95 % CI 1.00-1.07). Women who switched to a new provider upon arriving in their natal village had fewer facility-based prenatal (IRR = 0.86; 95 % CI 0.78-0.96) but more postnatal visits (IRR = 1.41; 95 % CI 1.06-1.87), regardless of how long they stayed.
For women who return to their natal home for childbirth, duration of stay and changing providers upon arrival are linked to differences in receipt of maternal healthcare. Increased attention to the needs of mobile women during the perinatal period is necessary to ensure they can participate in key birth customs while receiving adequate healthcare.
由于国家举措,印度农村地区的孕产妇健康状况有所改善,但在大多数社会人口群体中,医疗保健服务不足的情况仍然存在。围产期护理与临时分娩迁移(TCM)——回到娘家分娩和产后护理——这一普遍做法之间的联系仍未得到探索。
从瓦杜健康与人口监测点(HDSS)(马哈拉施特拉邦西部)1288名在2018 - 2022年期间分娩的妇女样本中收集有关迁移和健康访视的横断面数据。分娩迁移(暴露因素)通过三种方式进行分析:二元(是否有任何迁移)、连续(停留时间)和多维度(停留时间和提供者变更)。结果包括健康访视次数——包括医疗机构检查和社区卫生工作者的家访——以及早期产前护理的开始情况。使用了多变量泊松回归、负二项回归和逻辑回归。敏感性分析检查了回忆偏倚、迁移距离的影响以及模型设定错误。
迁移者和非迁移者在早期产前护理开始、医疗机构访视(怀孕前后)以及产前社区卫生工作者访视方面的结果相似。迁移者产后社区卫生工作者的访视次数较少(发病率比[IRR] = 0.80;95%置信区间[CI] 0.70 - 0.92)。在迁移者中,在娘家村庄停留时间较长与产前社区卫生工作者访视次数较少相关(IRR = 0.92;95% CI 0.88 - 0.96),但产后则不然(IRR = 1.03;95% CI 1.00 - 1.07)。到达娘家村庄后更换提供者的妇女产前医疗机构访视次数较少(IRR = 0.86;95% CI 0.78 - 0.96),但产后访视次数较多(IRR = 1.41;95% CI 1.06 - 1.87),无论她们停留多长时间。
对于回到娘家分娩的妇女,停留时间和到达后更换提供者与孕产妇医疗保健服务的接受情况差异有关。在围产期增加对流动妇女需求的关注,对于确保她们在参与关键生育习俗的同时能够获得足够的医疗保健是必要的。