Dell'Anna Antonio Maria, Grieco Domenico Luca, Dominedò Cristina, Cicetti Marta, Cisterna Irene, Festa Rossano, Lamacchia Rosa, Giannì Giuseppina, Filetici Nicoletta, Michi Teresa, Rossi Cristina, Alcaro Francesca Danila, Mele Alessandro, Rocchi Aurora, Del Prete Demetrio, Meluzio Maria Concetta, Tamburrelli Francesco Ciro, Rossi Marco, Antonelli Massimo
Department of Anesthesia and Intensive Care Medicine, Fondazione Policlinico Universitario "A. Gemelli" IRCCS, Università Cattolica del Sacro Cuore, L.Go F. Vito, 00168, Rome, Italy.
Department of Laboratory and Microbiological Analysis, Fondazione Policlinico Universitario "A. Gemelli" IRCCS, Università Cattolica del Sacro Cuore, Rome, Italy.
Ann Intensive Care. 2025 Apr 22;15(1):54. doi: 10.1186/s13613-025-01473-9.
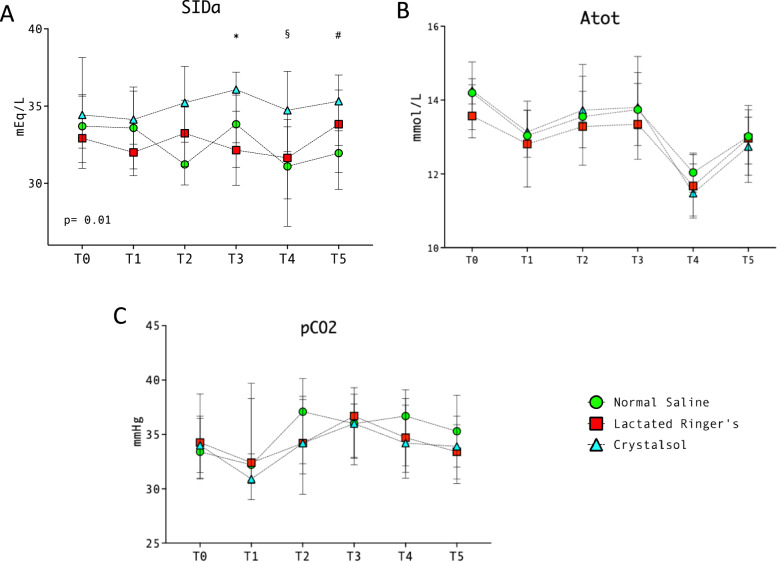
Stewart's acid-base theory states that, under isocapnic conditions, crystalloid infusion affects plasma pH due to changes in strong ion difference and total weak acid concentration: a comprehensive study also assessing renal response and hemodilution effects has not been conducted in humans. We aimed to evaluate Stewart's approach during crystalloid infusion in humans.
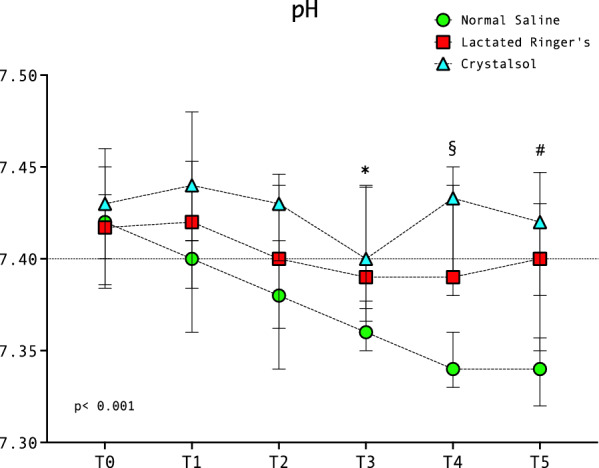
In this randomized trial, patients undergoing surgery with minimal blood losses were randomized to receive to normal saline (chloride content 154 mEq/L, strong ion difference 0 mEq/L), lactated Ringer's (chloride content 112 mEq/L, strong ion difference 29 mEq/L) or Crystalsol (chloride content 98 mEq/L, strong ion difference 50 mEq/L): patients received 10 ml/kg immediately after intubation, and 20 ml/kg after 2 h. Plasma/urinary acid-base and electrolytes were measured before study start and then at prespecified timepoints. The primary endpoint was pH one hour after the second fluid bolus: secondary outcomes included urinary/plasmatic electrolyte concentrations and strong ion difference during the study.
Forty-five patients were enrolled (15 in each group). The extent of hemodilution achieved with the first (median [Interquartile range]: saline 9% [6-15], Ringer's 7% [4-9], Crystalsol 8% [5-12]) and the second fluid bolus (saline 13% [5-17], Ringer's 12% [9-15], Crystalsol 15% [10-20]) was not different between groups (p = 0.39 and p = 0.19, respectively). Patients in saline group received more chloride (449 mEq [383-495]) vs. Ringer's (358 mEq [297-419]) and Crystalsol groups (318 mEq [240-366]) (p = 0.001). One hour after the second bolus, pH was lower in saline group (7.34 [7.32-7.36]) vs. Ringer's (7.40 [7.35-7.43) and Crystalsol groups (7.42 [7.38-7.44]) (both p < 0.01), since plasma chloride increased significantly over time in saline group but not in Ringer's and Crystalsol groups. Overall chloride urinary excretion was not different between study groups (saline 36 mEq [28-64], Ringer's 42 mEq [29-68], Crystalsol 44 mEq [27-56], p = 0.60) but, at the end of experiments, urinary chloride concentration was higher and diuresis was lower in saline group vs. Ringer's and Crystalsol groups (p = 0.01, p = 0.04, respectively).
Consistent with Stewart's approach, crystalloid solutions with high chloride content lower pH due to reduced strong ion difference, progressive hemodilutional acidosis and limited renal response to chloride load.
Registered on clinicaltrials.gov (NCT03507062) on April, 24th 2018.
斯图尔特酸碱理论指出,在等碳酸条件下,晶体液输注会因强离子差和总弱酸浓度的变化而影响血浆pH值:尚未在人体中进行过一项全面研究,同时评估肾脏反应和血液稀释效应。我们旨在评估人体晶体液输注过程中的斯图尔特方法。
在这项随机试验中,将失血极少的手术患者随机分为接受生理盐水(氯含量154 mEq/L,强离子差0 mEq/L)、乳酸林格液(氯含量112 mEq/L,强离子差29 mEq/L)或晶体溶液(氯含量98 mEq/L,强离子差50 mEq/L):患者在插管后立即接受10 ml/kg,2小时后接受20 ml/kg。在研究开始前以及预定时间点测量血浆/尿液酸碱和电解质。主要终点是第二次推注液体后1小时的pH值:次要结果包括研究期间尿液/血浆电解质浓度和强离子差。
共纳入45例患者(每组15例)。第一组(中位数[四分位间距]:生理盐水组9% [6 - 15],林格液组7% [4 - 9],晶体溶液组8% [5 - 12])和第二组推注液体(生理盐水组13% [5 - 17],林格液组12% [9 - 15],晶体溶液组15% [10 - 20])后达到的血液稀释程度在组间无差异(分别为p = 0.39和p = 0.19)。生理盐水组患者比林格液组(358 mEq [297 - 419])和晶体溶液组(318 mEq [240 - 366])接受了更多的氯(449 mEq [383 - 495])(p = 0.001)。第二次推注后1小时,生理盐水组的pH值(7.34 [7.32 - 7.36])低于林格液组(7.40 [7.35 - 7.43])和晶体溶液组(7.42 [7.38 - 7.44])(均p < 0.01),因为生理盐水组血浆氯随时间显著增加,而林格液组和晶体溶液组未增加。研究组间总体尿氯排泄无差异(生理盐水组36 mEq [28 - 64],林格液组42 mEq [29 - 68],晶体溶液组44 mEq [27 - 56],p = 0.60),但在实验结束时,生理盐水组的尿氯浓度较高,尿量低于林格液组和晶体溶液组(分别为p = 0.01,p = 0.04)。
与斯图尔特方法一致,高氯含量的晶体溶液由于强离子差降低、渐进性血液稀释性酸中毒和肾脏对氯负荷的反应有限而降低pH值。
于2018年4月24日在clinicaltrials.gov上注册(NCT03507062)。