Alnazari Nasser, Alanazi Omar Ibrahim, Alosaimi Muath Owaidh, Alanazi Ziyad Mohamed, Alhajeri Ziyad Mohammed, Alhussaini Khaled Mohammed, Alanazi Abdulkarim Mekhlif, Azzam Ahmed Y
Hepatobiliary Science and Organ Transplant Center, King Abdulaziz Medical City, Ministry of National Guard Health Affairs, Riyadh, Saudi Arabia.
King Abdullah International Medical Research Center (KAIMRC), Riyadh, Saudi Arabia.
BMC Nephrol. 2025 Apr 22;26(1):203. doi: 10.1186/s12882-025-04128-w.
Hospital readmission following renal transplantation significantly impacts patient outcomes and healthcare resources. While machine learning approaches offer promising solutions for risk prediction, their clinical application often lacks interpretability. We developed an explainable artificial intelligence (XAI) based supervised learning model to predict 30-day hospital readmission risk following renal transplantation.
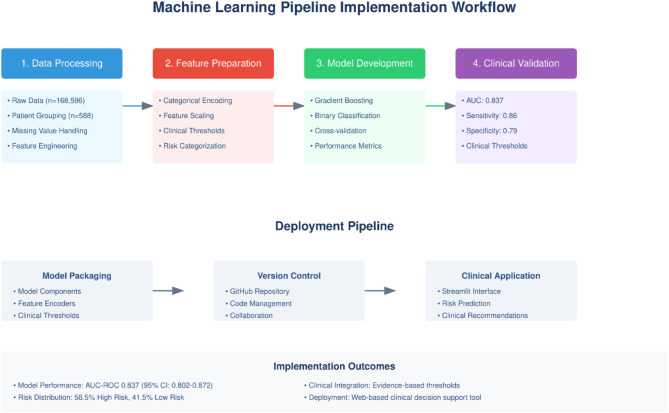
We conducted a retrospective analysis of 588 renal transplant recipients at King Abdullah International Medical Research Center, with a predominance of living donor transplants (85.2%, n = 500). Our methodology included a four-stage machine learning pipeline: data processing, feature preparation, model development using stratified 5-fold cross-validation, and clinical validation. Multiple algorithms were evaluated, with gradient boosting demonstrating superior performance. Model interpretability was achieved through dual-approach analysis using SHAP (SHapley Additive exPlanations) and LIME (Local Interpretable Model-agnostic Explanations).
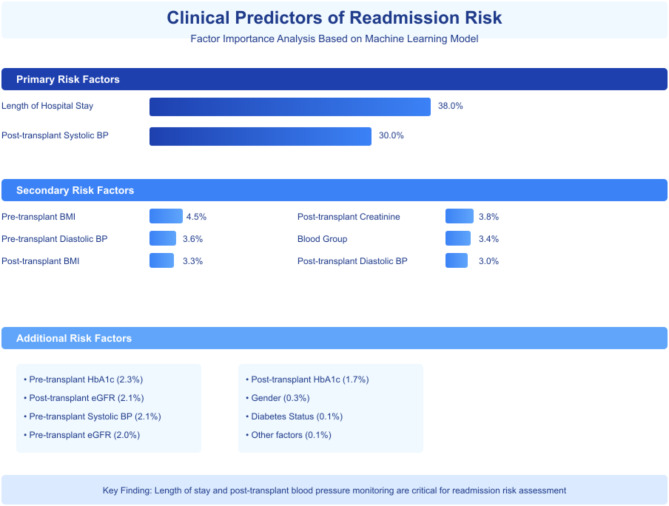
The gradient boosting model demonstrated strong performance (AUC 0.837, 95% CI: 0.802-0.872) with accuracy of 0.796 ± 0.050 and sensitivity of 0.388 ± 0.129. Length of hospital stay (38.0% contribution) and post-transplant systolic blood pressure (30.0% contribution) emerged as primary predictors, with differences between living and deceased donor subgroups. Pre-transplant BMI showed a higher importance in deceased donor recipients (12.6% vs. 2.6%), while HbA1c and eGFR were more impacting in living donor outcomes. The readmission rate in our cohort (88.9%, n = 523) was higher than previously reported ranges (18-47%), likely reflecting center-specific practices.
Our XAI-based machine learning model combines strong predictive performance with clinical interpretability, offering transplant physicians donor-specific risk stratification capabilities. The web-based implementation facilitates practical integration into clinical workflows. Given our single-center experience and high proportion of living donors, external validation across diverse transplant centers is essential before widespread implementation. Our approach establishes a framework for developing center-specific risk prediction tools in transplant medicine.
肾移植后的医院再入院对患者预后和医疗资源有显著影响。虽然机器学习方法为风险预测提供了有前景的解决方案,但其临床应用往往缺乏可解释性。我们开发了一种基于可解释人工智能(XAI)的监督学习模型,以预测肾移植后30天的医院再入院风险。
我们对阿卜杜拉国王国际医学研究中心的588名肾移植受者进行了回顾性分析,其中活体供体移植占多数(85.2%,n = 500)。我们的方法包括一个四阶段的机器学习流程:数据处理、特征准备、使用分层5折交叉验证的模型开发以及临床验证。评估了多种算法,梯度提升显示出卓越的性能。通过使用SHAP(SHapley加性解释)和LIME(局部可解释模型无关解释)的双方法分析实现了模型可解释性。
梯度提升模型表现出强大的性能(AUC 0.837,95% CI:0.802 - 0.872),准确率为0.796 ± 0.050,灵敏度为0.388 ± 0.129。住院时间(贡献38.0%)和移植后收缩压(贡献30.0%)成为主要预测因素,活体和 deceased 供体亚组之间存在差异。移植前BMI在 deceased 供体受者中显示出更高的重要性(12.6%对2.6%),而糖化血红蛋白和估算肾小球滤过率对活体供体结果的影响更大。我们队列中的再入院率(88.9%,n = 523)高于先前报道的范围(18 - 47%),这可能反映了中心特定的做法。
我们基于XAI的机器学习模型将强大的预测性能与临床可解释性相结合,为移植医生提供了供体特异性风险分层能力。基于网络的实施便于实际整合到临床工作流程中。鉴于我们的单中心经验和活体供体的高比例,在广泛实施之前,跨不同移植中心的外部验证至关重要。我们的方法为移植医学中开发中心特定的风险预测工具建立了一个框架。