Boughzala Mohamed Lotfi, Pereira Bruno, Ruivard Marc, Lobbes Hervé
Médecine Interne, Hôpital Estaing, Centre Hospitalier Universitaire de Clermont-Ferrand, 1 Place Lucie et Raymond Aubrac, Clermont-Ferrand, 63100, France.
Département de Biostatistiques, Direction de la Recherche Clinique et de l'Innovation, Centre Hospitalier Universitaire de Clermont-Ferrand, 28 Place Henri Dunant, Clermont-Ferrand, 63000, France.
BMC Gastroenterol. 2025 May 2;25(1):331. doi: 10.1186/s12876-025-03891-2.
In metabolic hyperferritinemia, most patients do not require bloodletting as the liver iron content is mildly increased. We aimed to develop a clinical predictive score of high liver iron content in metabolic hyperferritinemia to guide the prescription of magnetic resonance imaging of the liver.
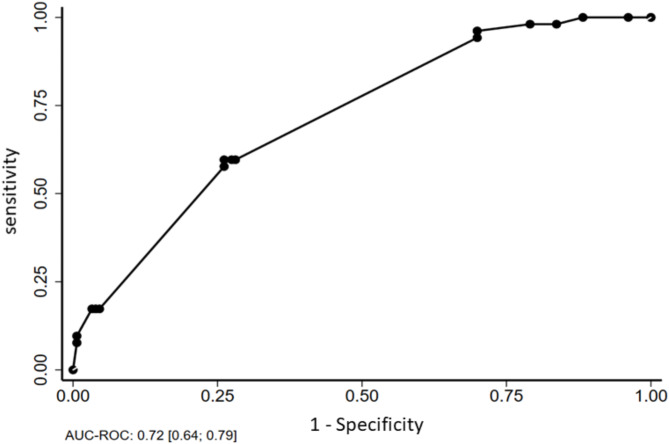
We conducted a single-center retrospective cohort study including consecutive patients with metabolic hyperferritinemia who underwent a liver iron content evaluation at diagnosis. Excessive alcohol consumption was an exclusion criterion. A multivariate analysis followed by a 1000 bootstrap replicate analysis with an expectation-maximization algorithm was used to identify the predictive factors of high liver iron content. A ROC curve analysis was built to study the performance of the score based on the odds-ratio provided by the multivariate analysis.
217 patients (180 men, mean age 57 years old) were included. Fifty-five patients (25%) had high liver iron content (≥ 100 µmol/g). In univariate analysis, a family history of hyperferritinemia requiring phlebotomies was associated with high LIC, as well as an increase of transferrin saturation > 45% (p < 0.001). In multivariate regression, a family history of hyperferritinemia (OR 6.15, CI95 [2.11-17.92]), increased ferritin level ≥ 600 µg/L (OR 5.53, CI95 [1.43-21.42]) and increased transferrin saturation ≥ 45% (OR 2.63, CI95 [1.32-5.23]) were significantly associated with high liver iron content. A 15-point predictive score (area-under-the-curve 0.72, CI95 [0.64-0.79], p < 0.001) was built, providing an OR of 4.17 (CI95 [2.15-8.07], p < 0.001) for high liver iron content (sensitivity 60%, specificity 97%, negative predictive value 84%).
in this pilot study, ferritin ≥ 600 µg/L, transferrin saturation ≥ 45% and a family history of hyperferritinemia requiring bloodletting provided a simple clinical score to predict high liver iron content in metabolic adult hyperferritinemia. The bootstrap analysis confirmed the robustness of our model.
在代谢性高铁蛋白血症中,大多数患者不需要放血治疗,因为其肝脏铁含量仅轻度升高。我们旨在制定一种代谢性高铁蛋白血症患者肝脏铁含量升高的临床预测评分系统,以指导肝脏磁共振成像检查的应用。
我们进行了一项单中心回顾性队列研究,纳入了诊断时接受肝脏铁含量评估的连续性代谢性高铁蛋白血症患者。排除大量饮酒者。采用多因素分析,随后使用期望最大化算法进行1000次重复抽样分析,以确定肝脏铁含量升高的预测因素。根据多因素分析提供的比值比构建ROC曲线,以研究该评分系统的性能。
共纳入217例患者(180例男性,平均年龄57岁)。55例患者(25%)肝脏铁含量升高(≥100 μmol/g)。单因素分析显示,需要放血治疗的高铁蛋白血症家族史与肝脏铁含量升高相关,转铁蛋白饱和度升高>45%也与之相关(p<0.001)。多因素回归分析显示,高铁蛋白血症家族史(比值比6.15,95%置信区间[2.11-17.92])、铁蛋白水平升高≥600 μg/L(比值比5.53,95%置信区间[1.43-21.42])和转铁蛋白饱和度升高≥%(比值比2.63,95%置信区间[1.32-5.23])与肝脏铁含量升高显著相关。构建了一个15分的预测评分系统(曲线下面积0.72,95%置信区间[中0.64-0.79],p<0.001),其预测肝脏铁含量升高的比值比为4.17(95%置信区间[2.15-8.07],p<0.001)(敏感性60%,特异性97%,阴性预测值84%)。
在这项初步研究中,铁蛋白≥600 μg/L、转铁蛋白饱和度≥45%以及需要放血治疗的高铁蛋白血症家族史可提供一个简单的临床评分系统,用于预测成年代谢性高铁蛋白血症患者的肝脏铁含量升高。重复抽样分析证实了我们模型的稳健性。