Aldabbour Belal, Elhissi Ahmed J H, Abudaqqa Hamza, Alqrinawi Jaser, Badran Mohammed, Sulaiman Mohammed, Alsoos Yousef, Altartour Yousef, Abulebda Mohammed, Muhaisen Mohammed, Alsafadi Omar, Assaf Zuhair
Faculty of Medicine, Islamic University of Gaza, P.O. Box 108, Gaza, State of Palestine.
BMC Health Serv Res. 2025 May 6;25(1):646. doi: 10.1186/s12913-025-12833-3.
Validation studies of prognostic models used in critical care have yet to be conducted in Palestine. The intense conflict in the Gaza Strip presents an opportunity to evaluate the performance of local ICUs and validate the performance of the MPM and SAPS models within a resource-limited and highly stressed healthcare system.
A prospective study conducted from October to December 2024 included all patients admitted to ICUs in three of the four critical care units operating in the Gaza Strip. Sociodemographic, clinical, physiological, and laboratory parameters were collected, along with information regarding the clinical course and ICU outcomes. The MPM-III and SAPS-III scores were calculated, and their discrimination and calibration were assessed using AUROC and the Hosmer-Lemeshow test, respectively. Furthermore, the difference between the predicted and actual mortality rates was visualized, and standardized mortality rates (SMR) were calculated. Except for the Hosmer-Lemeshow test, a p-value of less than 0.05 was deemed statistically significant. All statistical analyses were conducted using R Studio.
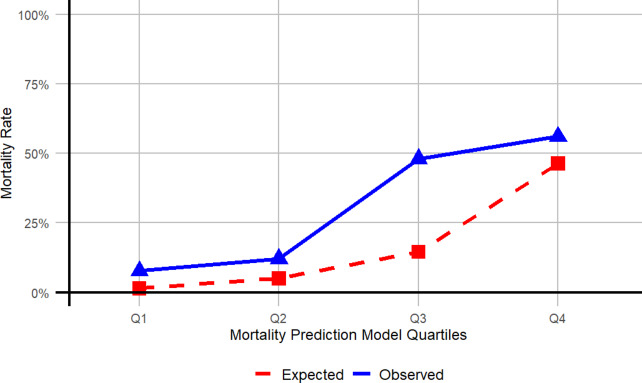
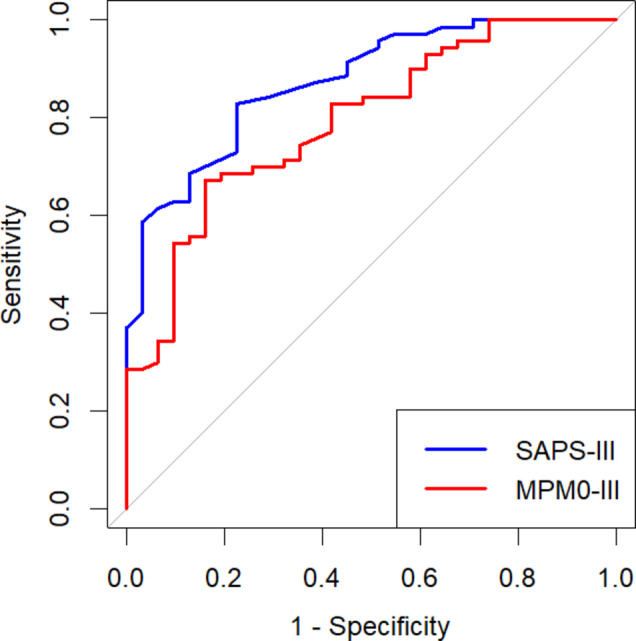
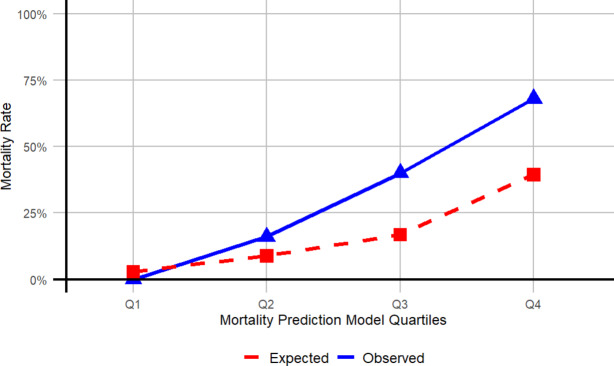
The cohort included 101 patients, of whom 72.27% were surgical cases and 58.41% were admitted from the ER. The ICU mortality rate was 30.69%. The median duration of ICU admission was four days [IQR 2-9] and was significantly longer for surgical cases than for medical cases. Physiological and laboratory parameters, along with interventions associated with higher mortality, included a lower GCS, burns, elevated leukocyte and platelet counts, lower PPO2, dysrhythmias, intracranial mass effect, and the need for mechanical ventilation or central venous catheterization. The predicted mortality rates were 16.63% for MPM0-III and 16.82% for SAPS-III. SMRs indicated that both models underestimated ICU mortality (SMR, MPM0-III 1.85; SAPS-III 1.83), with the discrepancy more likely to occur in high-risk patients. ROC curves demonstrated acceptable to good discriminatory power for both models (AUROC, MPM0-III 0.79 (95% CI 0.7-0.88); SAPS-III 0.87 (95% CI 0.80-0.94)). The Hosmer-Lemeshow test yielded statistically insignificant results for both models, indicating good calibration.
The outcomes of critical care units in the Gaza Strip during the studied period of the war were comparable to those of other hospitals in the West Bank and other LMICs without active conflicts. The MPM-III and SAPS-III demonstrated good discrimination and calibration, making them valid tools for enhancing ICU performance and improving resource utilization in the Gaza Strip.
巴勒斯坦尚未对重症监护中使用的预后模型进行验证研究。加沙地带的激烈冲突为评估当地重症监护病房的表现以及在资源有限且压力巨大的医疗系统中验证MPM和SAPS模型的表现提供了契机。
2024年10月至12月进行的一项前瞻性研究纳入了加沙地带四个重症监护病房中三个病房收治的所有患者。收集了社会人口统计学、临床、生理和实验室参数,以及有关临床病程和重症监护病房结局的信息。计算了MPM-III和SAPS-III评分,并分别使用AUROC和Hosmer-Lemeshow检验评估其辨别力和校准情况。此外,还直观展示了预测死亡率与实际死亡率之间的差异,并计算了标准化死亡率(SMR)。除Hosmer-Lemeshow检验外,p值小于0.05被视为具有统计学意义。所有统计分析均使用R Studio进行。
该队列包括101名患者,其中72.27%为外科病例,58.41%从急诊室收治。重症监护病房死亡率为30.69%。重症监护病房住院时间中位数为4天[四分位间距2 - 9],外科病例明显长于内科病例。生理和实验室参数以及与较高死亡率相关的干预措施包括格拉斯哥昏迷量表评分较低、烧伤、白细胞和血小板计数升高、动脉血氧分压较低、心律失常、颅内占位效应以及需要机械通气或中心静脉置管。MPM0 - III的预测死亡率为16.63%,SAPS - III为16.82%。标准化死亡率表明这两个模型均低估了重症监护病房死亡率(SMR,MPM0 - III为1.85;SAPS - III为1.83),差异在高危患者中更可能出现。ROC曲线显示这两个模型的辨别力均可接受至良好(AUROC,MPM0 - III为0.79(95%CI0.7 - 0.88);SAPS - III为0.87(95%CI0.80 - 0.94))。Hosmer-Lemeshow检验对两个模型均得出无统计学意义的结果,表明校准良好。
在所研究的战争期间,加沙地带重症监护病房的结局与约旦河西岸其他医院以及其他无冲突的低收入和中等收入国家的医院相当。MPM-III和SAPS-III表现出良好的辨别力和校准能力,使其成为提高加沙地带重症监护病房表现和改善资源利用的有效工具。