Sitefane Gilda Gondola, Essén Birgitta, Loquiha Osvaldo, Munguambe Khátia, Mariano Esmeralda, Ugarte William, Axemo Pia
Department of Women's and Children's Health, International Maternal Health and Migration Unit (IMHm), MTC-huset, Uppsala University, Dag Hammarskjölds Väg 14B, Uppsala, 752 37, Sweden.
Department of Mathematics and Informatics, Faculty of Science, Eduardo Mondlane University, Maputo, Mozambique.
BMC Health Serv Res. 2025 May 21;25(1):732. doi: 10.1186/s12913-025-12896-2.
Reducing maternal deaths is a critical public health concern. The Sustainable Development Goals (SDGs) aim to reduce maternal mortality globally to less than 70/100,000 live births by 2030. Mozambique has one of the highest maternal mortality rates in the world, at 233/100,000 live births. Of all maternal deaths, 11% are attributed to abortion. Mozambique decriminalized abortion in 2014 under certain conditions and approved clinical guidelines for service provision in 2016, aiming to reduce maternal deaths from unsafe abortion. This study assesses the availability, coverage, and utilization of facility-based voluntary termination of pregnancy (VTP) during the period 2016-2021 in Nampula province, northern Mozambique.
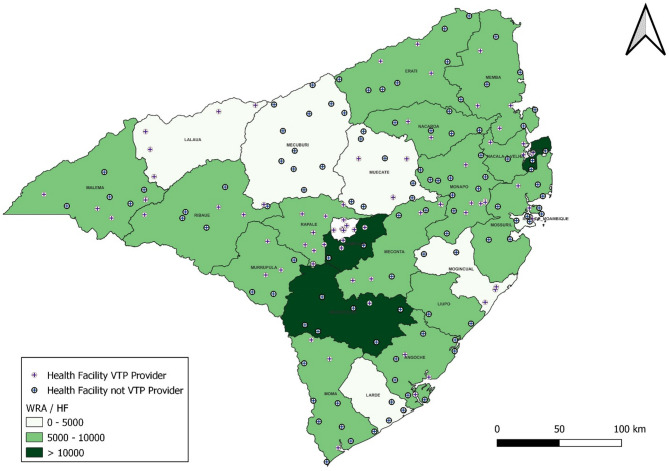
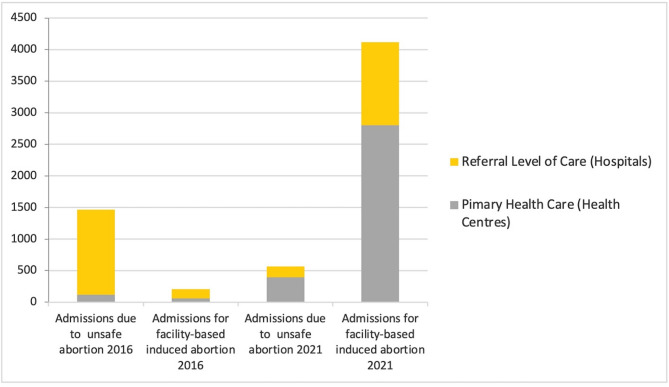
A descriptive quantitative study was performed, using secondary data analysis extracted from the national health monitoring information system (SIS-MA). Trends in the availability and utilization of VTP services were calculated from 2016 to 2021. The results were analysed while considering the geospatial distribution, coverage, and level of care of health facilities providing such services.
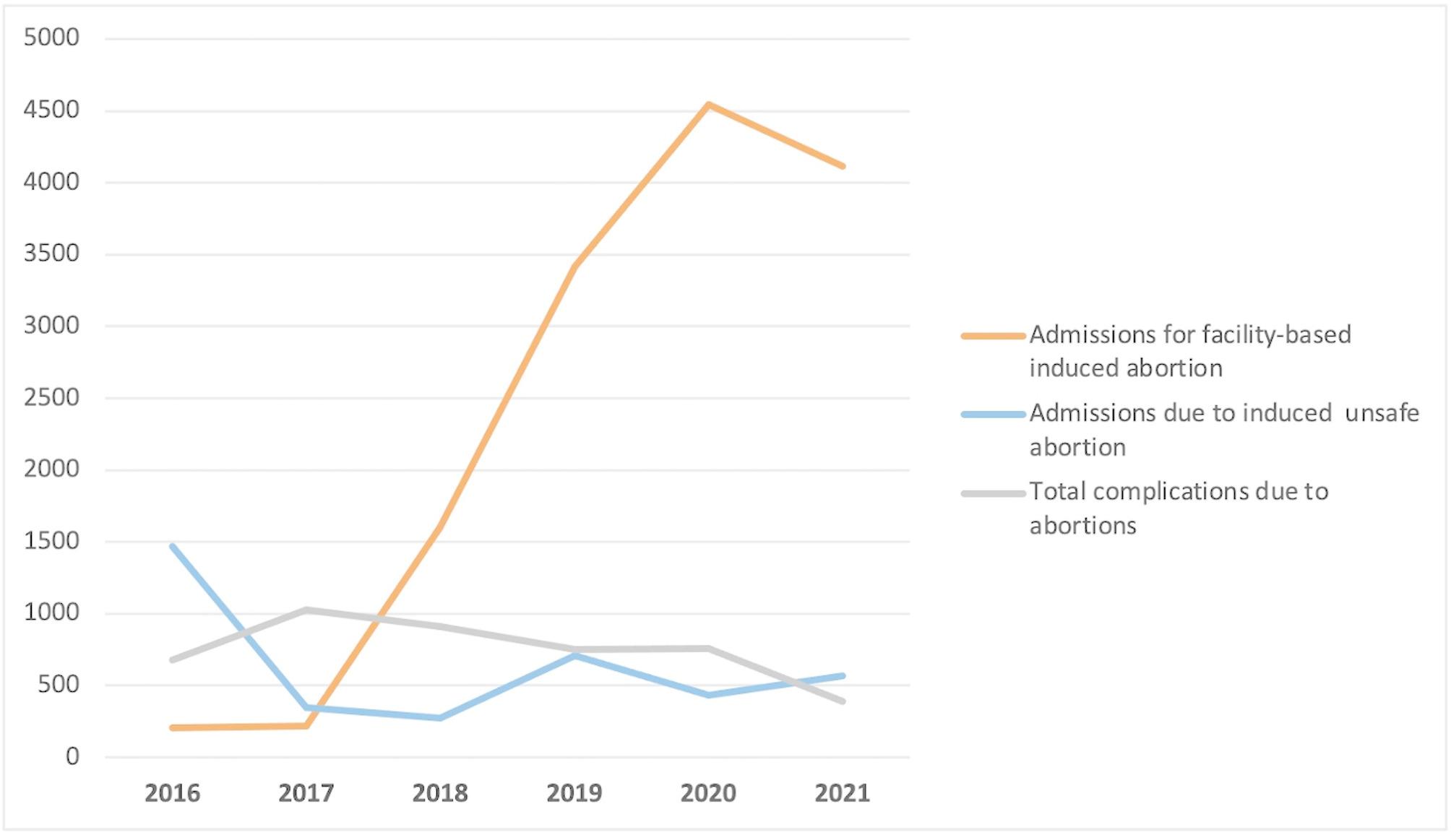
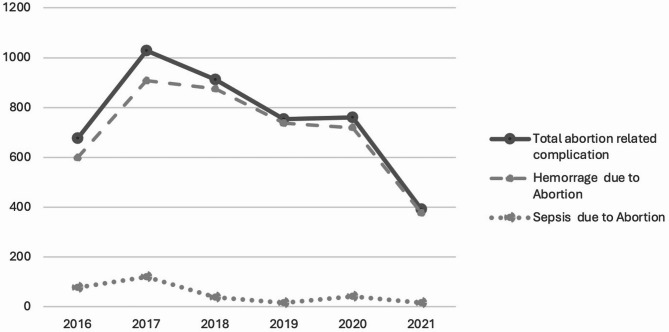
Utilization of VTP services significantly increased by 77% (p < 0.001) and complications related to unsafe abortion decreased by 23.5% (p = 0.018) during 2016-2021.
Despite the significant improvement in service availability and utilization, the geographic distribution and population coverage of public health facilities providing services remains uneven and limited to semi-urban and urban areas, leaving unsafe abortion as the only option for women in rural areas. Despite these challenges, the results of this study reinforce scientific evidence that decriminalization of VTP and expansion of services may significantly improve access to and utilization of facility-based VTP, holding great potential for decreasing unsafe abortion-related complications and deaths.
降低孕产妇死亡率是一项至关重要的公共卫生问题。可持续发展目标(SDGs)旨在到2030年将全球孕产妇死亡率降至每10万活产少于70例。莫桑比克是世界上孕产妇死亡率最高的国家之一,为每10万活产233例。在所有孕产妇死亡中,11%归因于流产。2014年,莫桑比克在某些条件下将流产合法化,并于2016年批准了服务提供的临床指南,旨在减少不安全流产导致的孕产妇死亡。本研究评估了2016 - 2021年期间莫桑比克北部楠普拉省基于设施的自愿终止妊娠(VTP)的可及性、覆盖率和利用率。
进行了一项描述性定量研究,使用从国家卫生监测信息系统(SIS - MA)提取的二手数据分析。计算了2016年至2021年VTP服务的可及性和利用率趋势。在分析结果时考虑了提供此类服务的卫生设施的地理空间分布、覆盖率和护理水平。
2016 - 2021年期间,VTP服务的利用率显著提高了77%(p < 0.001),与不安全流产相关的并发症减少了23.5%(p = 0.018)。
尽管服务的可及性和利用率有显著改善,但提供服务的公共卫生设施的地理分布和人口覆盖率仍然不均衡,且仅限于半城市和城市地区,这使得不安全流产成为农村地区妇女的唯一选择。尽管存在这些挑战,本研究结果强化了科学证据,即VTP合法化和服务扩展可能显著改善基于设施的VTP的可及性和利用率,对于减少与不安全流产相关的并发症和死亡具有巨大潜力。