Triplett Hunter, Winter Victoria, Leary Brandon, Lee Alexis, Sulkowski Kathryn, Kang Eugene
Kirk Kerkorian School of Medicine at University of Nevada Las Vegas, Las Vegas, Nevada.
Saint Mary's College of California. Moraga, California.
Clin Pract Cases Emerg Med. 2025 May;9(2):215-219. doi: 10.5811/cpcem.35488.
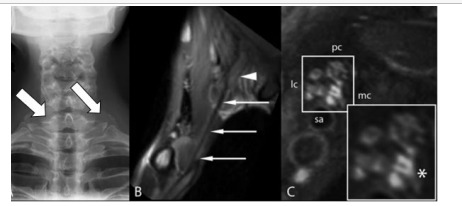
Thoracic outlet syndrome (TOS) is a diagnosis classifying upper extremity symptoms caused by compression of the neurogenic and vascular structures between the clavicle and first rib. It is important to promptly decompress these structures to prevent long-term deficits and poor patient outcomes. However, TOS often presents in unique ways with substantial symptom variance, making it difficult to identify, diagnose, and promptly treat. Compounding this, common diagnostic tools such as magnetic resonance imaging are not independently appropriate for a conclusive diagnosis of TOS. Patients with TOS can initially present acutely due to symptom exacerbations or emergent situations, necessitating multimodal diagnostic methods and early TOS recognition to improve patient outcomes, particularly in emergency department (ED) settings.
A 22-year-old male presented with chronic symptoms of numbness and weakness in his right hand in addition to chest pain that radiated into his right elbow, along with a diminished right radial pulse. The patient also suffered from acute symptomatic exacerbations of total arm asthenia, paresthesia, and what the patient described as "an intensely cold hand" during football practice. He was eventually treated with a right first-rib resection to decompress the brachial plexus, which resulted in complete symptom resolution and recovery.
Due to the serious long-term complications associated with uncorrected brachial plexus compression and the fact that TOS patients can initially present to ED settings with acute exacerbations, it is important for emergency clinicians to be able to recognize and either treat or appropriately refer patients for treatment. The ED is equipped to enable physicians to perform a comprehensive diagnostic assessment because they often have access to the diagnostic modalities necessary for diagnosing thoracic outlet syndrome.
胸廓出口综合征(TOS)是一种对因锁骨与第一肋骨之间的神经和血管结构受压而导致上肢症状进行分类的诊断。及时对这些结构进行减压以防止长期功能缺损和不良患者预后非常重要。然而,TOS常以独特方式呈现,症状差异很大,这使得识别、诊断和及时治疗变得困难。更复杂的是,诸如磁共振成像等常见诊断工具并不适合独立用于TOS的确诊。TOS患者最初可能因症状加重或紧急情况而急性发病,因此需要多模式诊断方法和早期TOS识别来改善患者预后,尤其是在急诊科(ED)环境中。
一名22岁男性除了有放射至右肘部的胸痛外,还伴有右手慢性麻木和无力症状,右侧桡动脉搏动减弱。该患者在足球训练期间还出现了全臂乏力、感觉异常以及患者描述为“手部剧痛”的急性症状加重。他最终接受了右侧第一肋骨切除术以减压臂丛神经,症状完全缓解并康复。
由于未纠正的臂丛神经受压会导致严重的长期并发症,且TOS患者最初可能以急性加重的形式出现在急诊科,急诊临床医生能够识别并治疗或适当转诊患者进行治疗非常重要。急诊科具备让医生进行全面诊断评估的条件,因为他们通常可以使用诊断胸廓出口综合征所需的诊断方法。