Kaplan Sydney, da Cruz Gastao Lima, Madamanchi Chaitanya, Murthy Venkatesh L, Swanson Scott, Hamilton Jesse, Seiberlich Nicole
Department of Biomedical Engineering, University of Michigan, Ann Arbor, Michigan, USA.
Department of Radiology, University of Michigan, Ann Arbor, Michigan, USA.
Magn Reson Med. 2025 Oct;94(4):1500-1513. doi: 10.1002/mrm.30580. Epub 2025 May 23.
To develop a cardiac MR fingerprinting (cMRF) approach using deep image prior reconstruction (DIP) to simultaneously map T, T, and T, and assess T in healthy subjects and patients with areas of enhancement on late gadolinium enhancement.
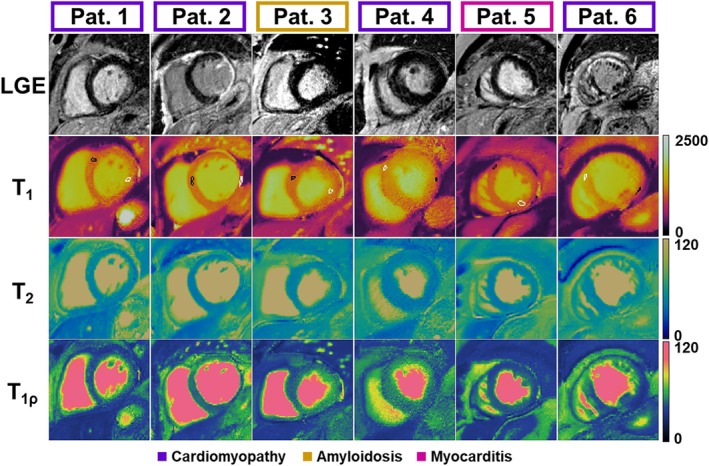
A 2D electrocardiogram-triggered cMRF sequence was developed to measure T, T, and T simultaneously. DIP reconstruction was evaluated for noise and artifact reduction compared to a low-rank reconstruction. Measurements were assessed in simulation and phantom for accuracy. T-cMRF maps were generated in 10 healthy subjects and six patients under evaluation for cardiomyopathy, myocarditis, and amyloidosis receiving gadolinium-based contrast agent-enhanced CMR at 1.5 T.
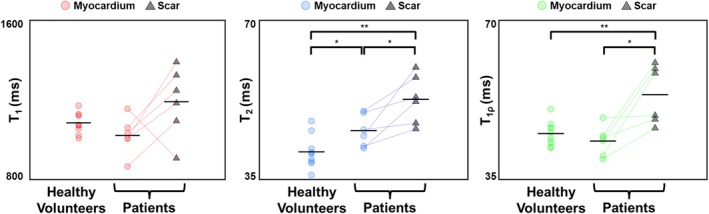
T-cMRF maps showed excellent agreement with ground truth (RMS error = 3.0% ± 5.3%) and conventional methods (R = 0.99) in simulations and phantom experiments. Measured values in healthy subjects were consistent with literature (T = 1051 ± 63 ms, T = 41.4 ± 3.3 ms, and T = 45.5 ± 2.4 ms). DIP reconstruction reduced noise, indicated by lower coefficient of variation (Δ = 4.7), compared to low-rank reconstruction. Mean differences of 10.2 ms (p = 0.02) in T and 6.9 ms in T maps were observed between areas of enhancement on late gadolinium enhancement and normal-appearing myocardium in patients. Within individual patients, significant differences (p < 0.01) in T, T, and T were observed between American Heart Association segments with and without contrast enhancement.
The proposed T-cMRF sequence using DIP reconstruction enables simultaneous quantification of T, T, and T with decreased coefficient of variation compared to low-rank reconstruction. Simulation and phantom studies show good agreement with references. In vivo measurements were made in healthy subjects, and areas of contrast enhancement in patients showed elevated T and T relative to remote myocardium.
开发一种使用深度图像先验重建(DIP)的心脏磁共振指纹图谱(cMRF)方法,以同时绘制T1、T2和T2*图谱,并评估健康受试者以及晚期钆增强出现强化区域的患者的T1值。
开发了一种二维心电图触发的cMRF序列,以同时测量T1、T2和T2*。与低秩重建相比,评估了DIP重建在降低噪声和伪影方面的效果。在模拟和体模中评估测量的准确性。在1.5 T下,对10名健康受试者和6名正在接受基于钆造影剂增强CMR评估的心肌病、心肌炎和淀粉样变性患者生成T1-cMRF图谱。
在模拟和体模实验中,T1-cMRF图谱与真实值(均方根误差 = 3.0% ± 5.3%)和传统方法(R = 0.99)显示出极好的一致性。健康受试者的测量值与文献一致(T1 = 1051 ± 63 ms,T2 =41.4 ± 3.3 ms,T2* = 45.5 ± 2.4 ms)。与低秩重建相比,DIP重建降低了噪声,变异系数更低(Δ = 4.7)表明了这一点。在患者中,晚期钆增强的强化区域与正常心肌区域之间的T1图谱平均差异为10.2 ms(p = 0.02),T2图谱平均差异为6.9 ms。在个体患者中,美国心脏协会有造影剂增强和无造影剂增强节段之间的T1、T2和T2*存在显著差异(p < 0.01)。
所提出的使用DIP重建的T1-cMRF序列能够同时定量T1、T2和T2*,与低秩重建相比变异系数降低。模拟和体模研究与参考值显示出良好的一致性。在健康受试者中进行了体内测量,患者的造影剂增强区域相对于远隔心肌显示出T1和T2升高。