Veronese Giacomo, Meani Paolo, Sirico Domenico, Di Salvo Giovanni, Ammirati Enrico, Varrica Alessandro, Di Dedda Umberto, Bianchi Paolo, Isgrò Giuseppe, Giamberti Alessandro, Aloisio Tommaso, Dickstein Marc, Bonanomi Ezio, Alsoufi Bahaaldin, Thiagarajan Ravi R, Alexander Peta M A, McMullan D Michael, Barbaro Ryan P, MacLaren Graeme, Ranucci Marco, Kapur Navin K, Lorusso Roberto
Pediatric Intensive Care Unit, ASST Papa Giovanni XXIII, Bergamo, Italy.
Department of Cardiothoracic Surgery, Heart and Vascular Centre, Maastricht University Medical Centre, Maastricht, The Netherlands.
ESC Heart Fail. 2025 Aug;12(4):2711-2725. doi: 10.1002/ehf2.15325. Epub 2025 May 26.
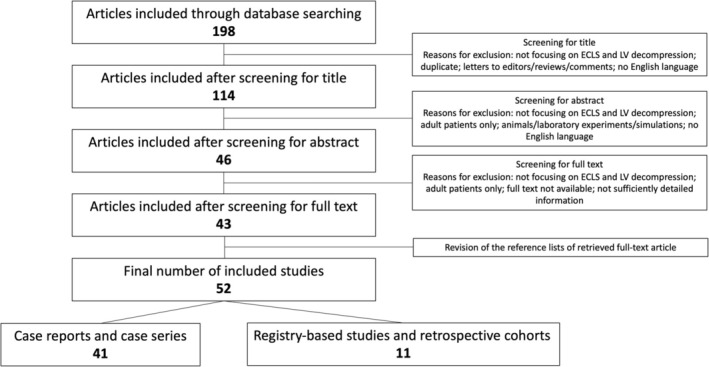
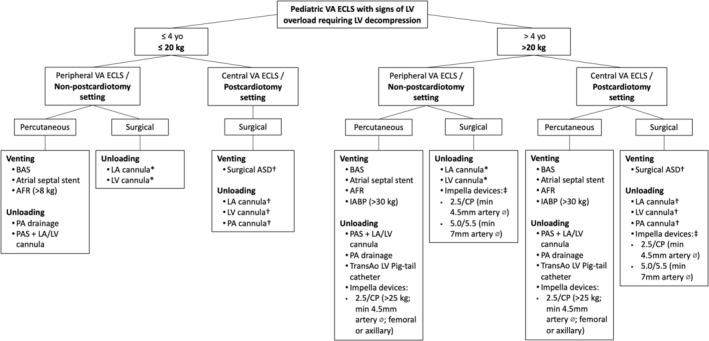
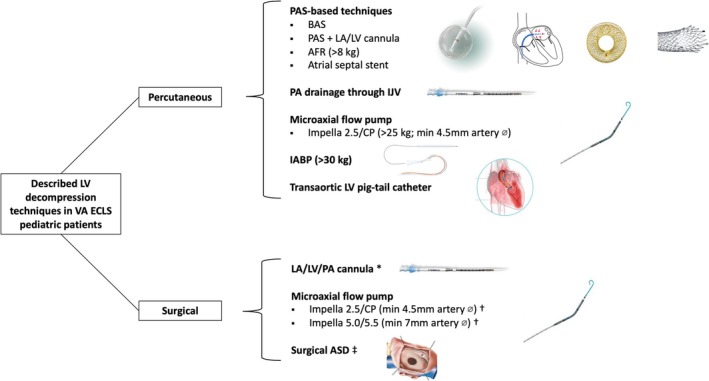
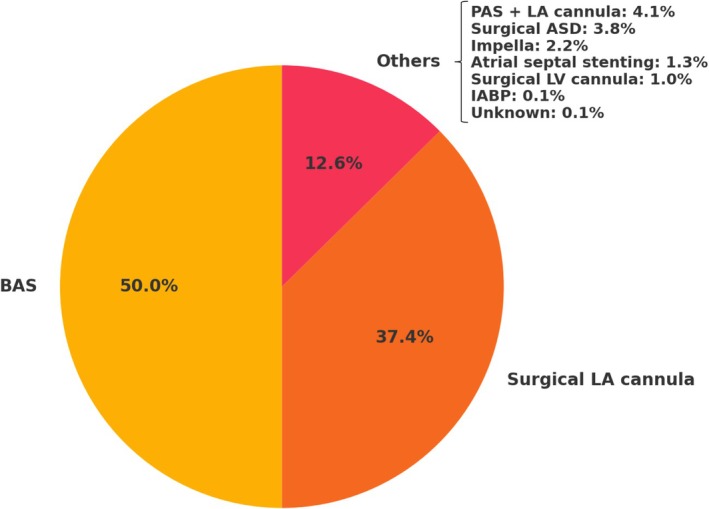
Veno-arterial extracorporeal life support (VA ECLS) is crucial for neonatal and paediatric patients with severe circulatory collapse but may cause left ventricular (LV) overload, affecting myocardial recovery and causing complications. Evidence on optimal LV decompression strategies in paediatric patients remains limited. We conducted a systematic review following PRISMA guidelines, including articles published between 1993 and 2024 focused on VA ECLS and LV decompression in patients under 18 years of age. The review included 11 retrospective cohorts and registry-based studies (2012-2024), totalling 1222 paediatric patients undergoing decompression. Patient demographics, initial diagnoses and VA ECLS settings were heterogeneous. The prevalence of LV decompression ranged from 46.6% in post-cardiotomy to 10.5% in non-post-cardiotomy peripheral VA ECLS cases. Most patients (57.1%) were supported with peripheral VA ECLS, and the majority (57.4%) underwent percutaneous decompression, whereas surgical approaches predominated in post-cardiotomy central VA ECLS. Balloon atrial septostomy (BAS) was the most frequent technique (50%), followed by surgically placed left atrial cannula (37.4%). Thirteen case series (70 patients) and 28 case reports (28 patients) were also reviewed. Substantial variability in LV decompression strategies exists based on age and clinical scenario. PAS-based techniques were more common in younger patients on peripheral VA ECLS while older children often underwent different strategies. Surgical approaches were preferred in central VA ECLS, particularly in the post-cardiotomy setting. Procedural safety varied by technique. While PAS-based strategies such as BAS generally showed low complication rates, adverse events like arrhythmia, bleeding and cardiac perforation were reported in 7%-9% of cases. Surgical LA cannulation was associated with higher bleeding risk. Impella use was linked to haemolysis (50%) and major bleeding (20%). Comparative data highlight that each technique carries distinct procedural risks and complication profiles. In conclusion, LV decompression during paediatric VA ECLS remains technically challenging and variably adopted. Its benefit appears more consistent in the post-cardiotomy setting, where improved survival and reduced adverse outcomes were observed. Given the lack of standardization, further prospective studies and collaborative registries are essential to guide strategy selection, timing and risk-benefit balance, particularly in such a vulnerable population.
静脉-动脉体外生命支持(VA ECLS)对于患有严重循环衰竭的新生儿和儿科患者至关重要,但可能导致左心室(LV)负荷过重,影响心肌恢复并引发并发症。关于儿科患者最佳左心室减压策略的证据仍然有限。我们按照PRISMA指南进行了一项系统综述,纳入了1993年至2024年发表的聚焦于18岁以下患者的VA ECLS和左心室减压的文章。该综述包括11项回顾性队列研究和基于注册登记的研究(2012 - 2024年),共有1222名接受减压的儿科患者。患者的人口统计学特征、初始诊断和VA ECLS设置各不相同。左心室减压的发生率在心脏手术后的患者中为46.6%,在非心脏手术后的外周VA ECLS病例中为10.5%。大多数患者(57.1%)接受外周VA ECLS支持,且大多数(57.4%)接受经皮减压,而在心脏手术后的中心VA ECLS中手术方法占主导。球囊房间隔造口术(BAS)是最常用的技术(50%),其次是手术放置的左心房插管(37.4%)。还对13个病例系列(70例患者)和28个病例报告(28例患者)进行了综述。基于年龄和临床情况,左心室减压策略存在很大差异。基于PAS的技术在接受外周VA ECLS的较年轻患者中更常见,而年龄较大的儿童通常采用不同的策略。手术方法在中心VA ECLS中更受青睐,尤其是在心脏手术后的情况下。不同技术的操作安全性各不相同。虽然基于PAS的策略如BAS通常显示出较低的并发症发生率,但在7% - 9%的病例中报告了心律失常、出血和心脏穿孔等不良事件。手术左心房插管与较高的出血风险相关。使用Impella与溶血(50%)和大出血(20%)有关。比较数据表明,每种技术都有独特的操作风险和并发症特征。总之,儿科VA ECLS期间的左心室减压在技术上仍然具有挑战性,且采用情况各不相同。其益处似乎在心脏手术后的情况下更为一致,在该情况下观察到生存率提高和不良后果减少。鉴于缺乏标准化,进一步的前瞻性研究和协作注册对于指导策略选择、时机和风险效益平衡至关重要,尤其是在这样一个脆弱的人群中。