Luo Jinfeng, Liu Jing, Lin Hongfu, Yang Yang, Chen Caihong, Chen Jianping, Zhong Han, Zhang Shipao
Department of Cardiology, The Second Hospital of Sanming, Sanming, Fujian, China.
Department of Critical Care Medicine, The Second Hospital of Sanming, Sanming, Fujian, China.
Front Med (Lausanne). 2025 May 9;12:1550053. doi: 10.3389/fmed.2025.1550053. eCollection 2025.
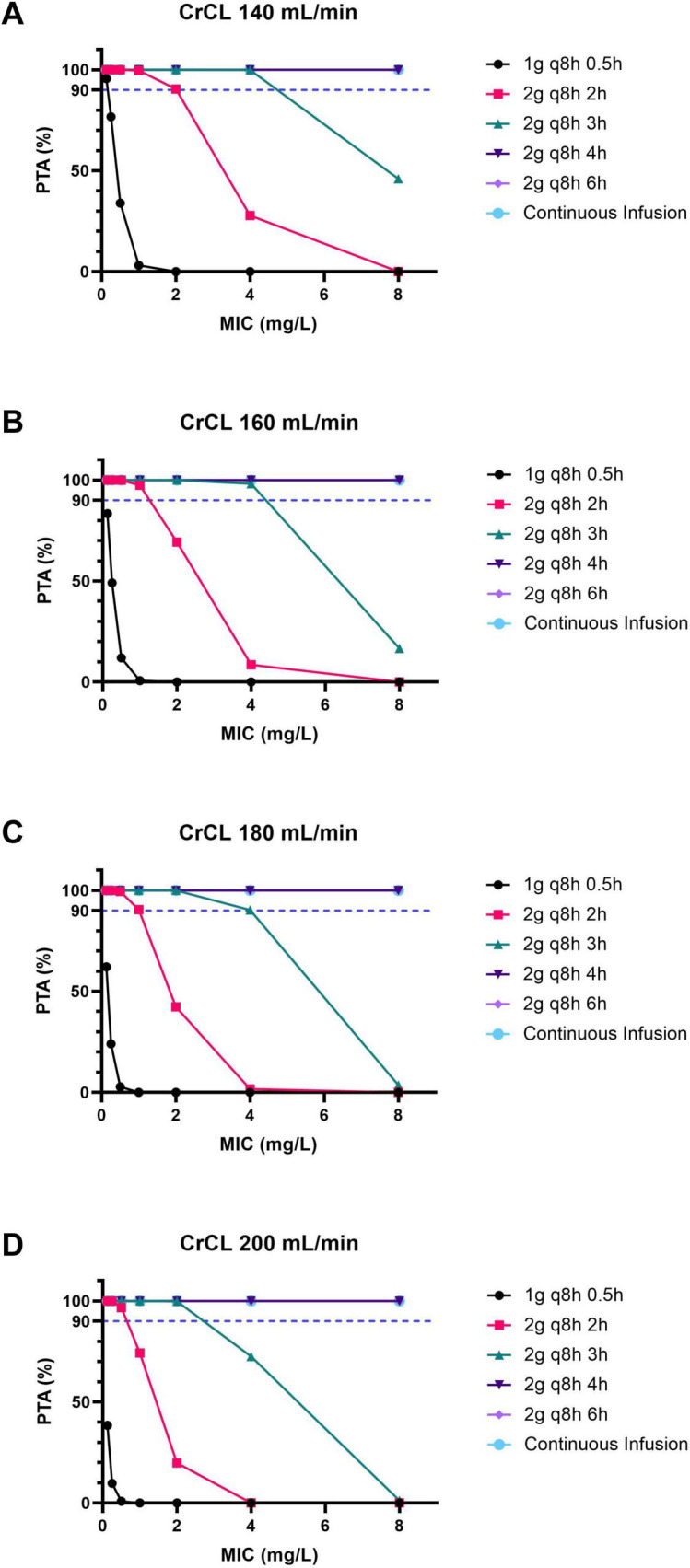
The pharmacokinetics of meropenem are significantly altered in patients with augmented renal clearance (ARC), resulting in suboptimal plasma concentrations. The objective of this study is to investigate the efficacy of different meropenem regimens in critically ill patients with ARC. To this end, Monte Carlo simulations were conducted. The probability of target attainment (PTA) and the cumulative fraction of response (CFR) were evaluated with consideration of the minimal inhibitory concentration (MIC) breakpoint according to the Clinical and Laboratory Standards Institute (CLSI). The findings of this study demonstrate that meropenem administered at a dosage of 2 every 8 h (q8 h) 2/3 h to critically ill patients with ARC [creatinine clearance (CrCL) of 140-200 mL/min] results in ≥ 90% PTA (100% T > MIC) for lower MICs (≤ 2 mg/L). However, for higher MICs (4-8 mg/L), the administration of intensified regimens (2 g q8 h 4/6 h or continuous infusion) was necessary. The CFR analysis confirmed ≥ 90% target attainment for with regimens meropenem 2 g q8 h 2-6 h or continuous infusion, but not for or , regardless of regimen. For resistant (4 < MIC ≤ 8), prolonged (4-6 h) or continuous infusions are recommended. For and , alternative or combination therapies are advised due to insufficient PK/PD target attainment with meropenem monotherapy. The findings emphasize the importance of individualized dosing strategies in ARC patients, considering meropenem's distinctive PK/PD characteristics, the pathogen's MIC, and renal function, in order to effectively manage resistant Gram-negative infections while optimizing clinical outcomes.
肾功能增强(ARC)患者美罗培南的药代动力学显著改变,导致血浆浓度不理想。本研究的目的是调查不同美罗培南给药方案对重症ARC患者的疗效。为此进行了蒙特卡洛模拟。根据临床和实验室标准协会(CLSI)的标准,考虑最低抑菌浓度(MIC)折点,评估达到目标概率(PTA)和累积反应分数(CFR)。本研究结果表明,对于ARC的重症患者[肌酐清除率(CrCL)为140 - 200 mL/min],每8小时(q8h)2g、输注2/3小时的美罗培南给药方案,对于较低MIC(≤2mg/L)可实现≥90%的PTA(100%T>MIC)。然而,对于较高MIC(4 - 8mg/L),则需要强化给药方案(每8小时2g、输注4/6小时或持续输注)。CFR分析证实,美罗培南2g q8h 2 - 6小时或持续输注方案可实现≥90%的目标达成率,但无论何种方案,对于[具体情况未明确,原文此处表述不完整]或[具体情况未明确,原文此处表述不完整]均未实现。对于耐药菌(4 < MIC ≤ 8),建议延长输注时间(4 - 6小时)或持续输注。对于[具体情况未明确,原文此处表述不完整]和[具体情况未明确,原文此处表述不完整],由于美罗培南单药治疗的药代动力学/药效学(PK/PD)目标达成不足,建议采用替代或联合治疗。这些发现强调了在ARC患者中个体化给药策略的重要性,要考虑美罗培南独特的PK/PD特征、病原体的MIC和肾功能,以便在优化临床结局的同时有效管理耐药革兰氏阴性菌感染。