Department of Nephrology, Charité Universitätsmedizin Berlin, Berlin, Germany.
Service de Néphrologie, Dialyse, Aphérèses et Transplantation, CHU Grenoble Alpes, Grenoble, France.
Transpl Int. 2022 Mar 21;35:10225. doi: 10.3389/ti.2021.10225. eCollection 2022.
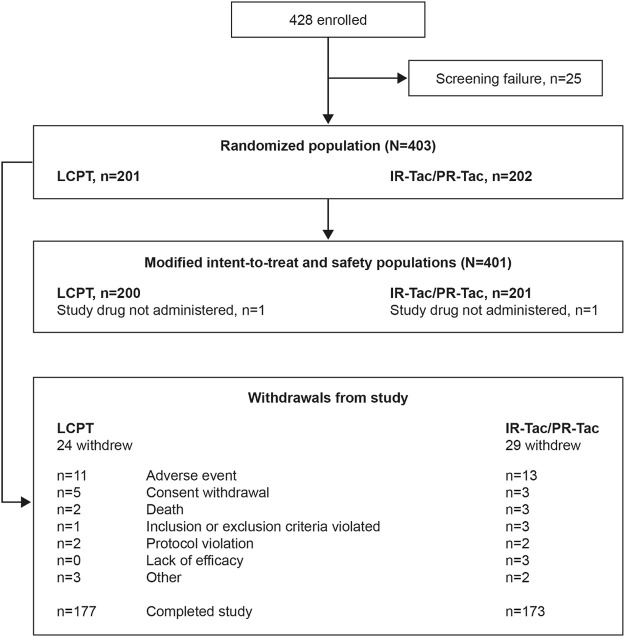
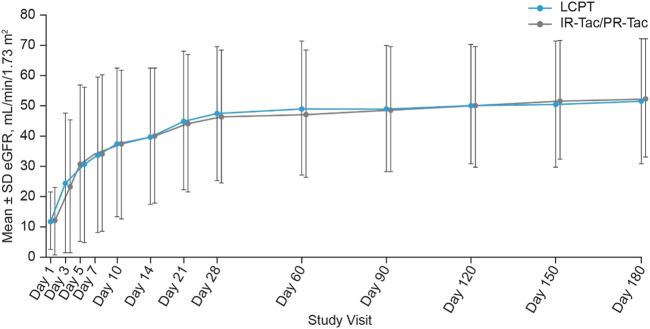
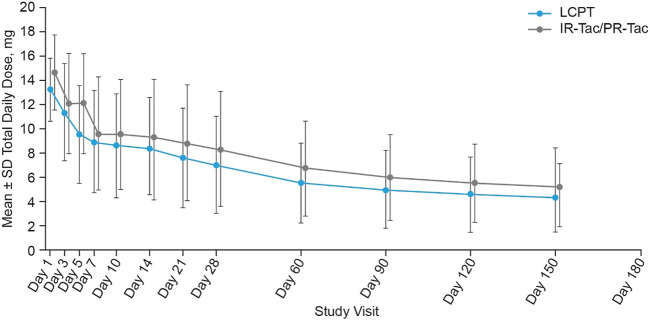
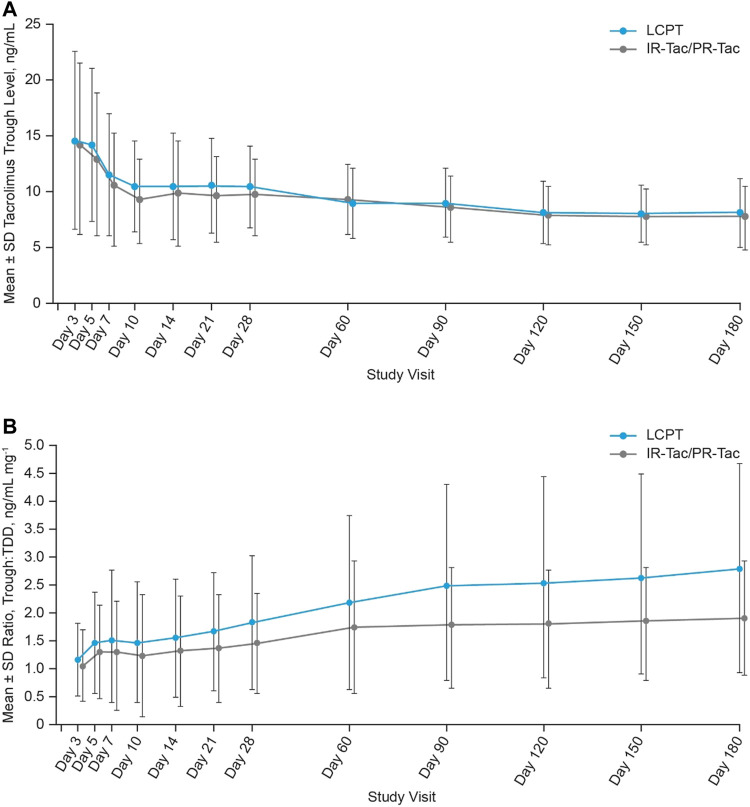
Tacrolimus is the calcineurin inhibitor of choice for preventing acute rejection episodes in kidney transplant patients. However, tacrolimus has a narrow therapeutic range that requires regular monitoring of blood concentrations to minimize toxicity. A new once-daily tacrolimus formulation, LCP-tacrolimus (LCPT), has been developed, which uses MeltDose™ drug-delivery technology to control drug release and enhance overall bioavailability. Our study compared dosing of LCPT with current standard-of-care tacrolimus [immediate-release tacrolimus (IR-Tac) or prolonged-release tacrolimus (PR-Tac)] during the 6 months following kidney transplantation. Comparisons of graft function, clinical outcomes, safety, and tolerability for LCPT versus IR-Tac/PR-Tac were also performed. Standard immunological risk patients with end-stage renal disease who had received a kidney transplant were randomized (1:1) to LCPT (N = 200) or IR-Tac/PR-Tac (N = 201). Least squares (LS) mean tacrolimus total daily dose from Week 3 to Month 6 was significantly lower for LCPT than for IR-Tac/PR-Tac. Although LS mean tacrolimus trough levels were significantly higher for LCPT than IR-Tac/PR-Tac, tacrolimus trough levels remained within the standard reference range for most patients. There were no differences between the groups in treatment failure measures or safety profile. LCPT can achieve similar clinical outcomes to other tacrolimus formulations, with a lower daily dose. https://clinicaltrials.gov/, identifier NCT02432833.
他克莫司是预防肾移植患者急性排斥反应的首选钙调磷酸酶抑制剂。然而,他克莫司的治疗窗较窄,需要定期监测血药浓度以最大程度地降低毒性。一种新的每日一次的他克莫司制剂,LCP-他克莫司(LCPT),已经开发出来,它使用 MeltDose™药物输送技术来控制药物释放并提高整体生物利用度。我们的研究比较了肾移植后 6 个月内 LCPT 与当前标准治疗的他克莫司[普通释放他克莫司(IR-Tac)或延长释放他克莫司(PR-Tac)]的剂量。还比较了 LCPT 与 IR-Tac/PR-Tac 在移植肾功能、临床结局、安全性和耐受性方面的差异。接受肾移植的终末期肾病标准免疫风险患者被随机(1:1)分为 LCPT(N=200)或 IR-Tac/PR-Tac(N=201)组。从第 3 周到第 6 个月的 LS 均值他克莫司总日剂量,LCPT 显著低于 IR-Tac/PR-Tac。尽管 LCPT 的 LS 均值他克莫司谷浓度显著高于 IR-Tac/PR-Tac,但大多数患者的他克莫司谷浓度仍在标准参考范围内。两组在治疗失败指标或安全性方面无差异。LCPT 可以达到与其他他克莫司制剂相似的临床结果,且日剂量更低。https://clinicaltrials.gov/,注册号 NCT02432833。