Ebinger Joseph E, Gupta Aakriti, Huang Tzu Yu, Kelley Marcella A, Thompson Christin, Platanis Maria, Cheng Susan
Department of Cardiology Smidt Heart Institute, Cedars-Sinai Medical Center Los Angeles CA USA.
Edwards Lifesciences Irvine CA USA.
J Am Heart Assoc. 2025 Jun 3;14(11):e041148. doi: 10.1161/JAHA.125.041148. Epub 2025 May 29.
Despite the slowly progressive nature of aortic stenosis, a proportion of aortic valve replacements (AVRs) still occur on an urgent/emergent basis. We sought to characterize the predictors, outcomes, and potential opportunities to prevent urgent/emergent AVRs.
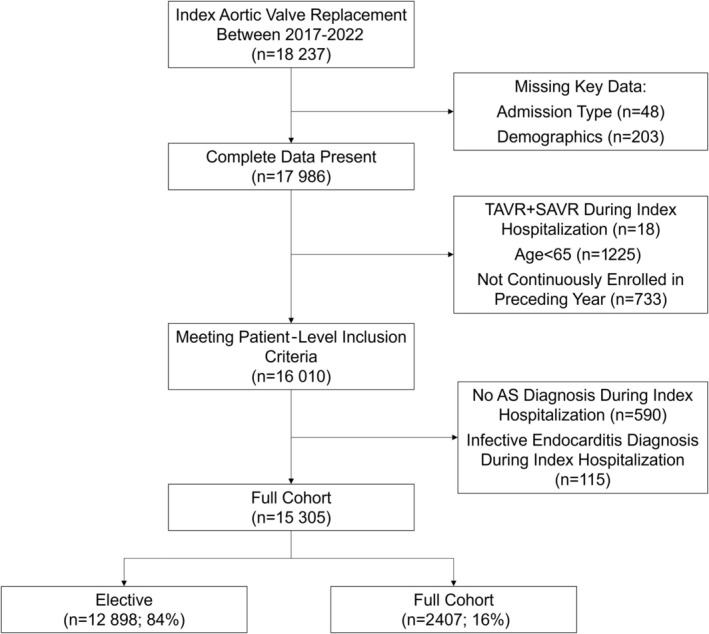
We analyzed Medicare data to identify patients undergoing AVRs from 2017 to 2022. We used multivariable regression to identify factors associated with nonelective AVRs; we also examined the association of nonelective AVRs with clinical outcomes and health care costs.
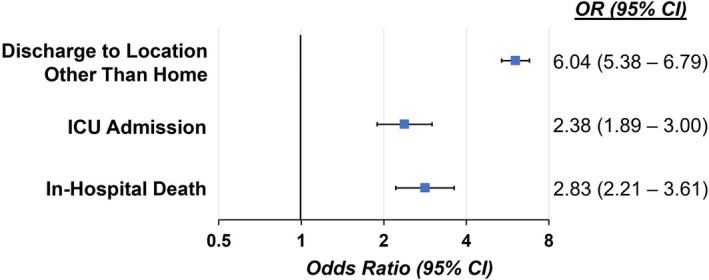
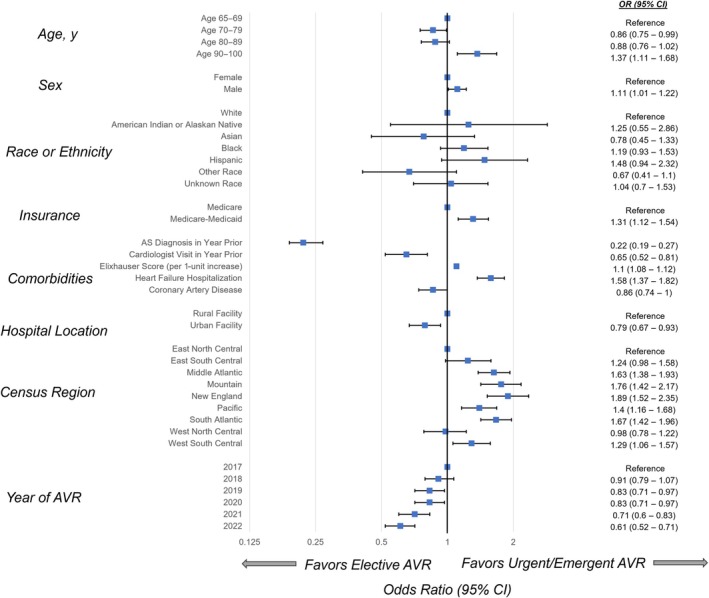
In total, 15 305 patients (16% urgent/emergent) underwent AVR during the study period. Compared with patients undergoing elective AVRs, those receiving urgent/emergent AVRs were more frequently of Black race or Hispanic ethnicity, and less likely to have received a diagnosis of aortic stenosis, despite 91.7% having seen a cardiologist or primary care provider in the prior year. In multivariable-adjusted analyses, dual Medicare-Medicaid enrollment, male sex, and recent heart failure hospitalization were associated with increased risk for urgent/emergent AVR; conversely, recent aortic stenosis diagnosis and cardiologist visit were associated with lower odds of urgent/emergent AVR. In turn, urgent/emergent compared with elective AVR increased risk for in-hospital death, intensive care unit admission, and discharge to a facility versus home, in addition to longer lengths of stay and higher health care costs.
Urgent/emergent AVR occurs more frequently among Black, Hispanic, and dual Medicare-Medicaid-eligible patients. Nonelective AVR is also associated with worse hospital outcomes as well as greater health care costs. Importantly, variable timing in diagnosis of aortic stenosis appears to be a key determinant; thus, augmented screening efforts may improve outcomes and reduce disparities.
尽管主动脉瓣狭窄具有缓慢进展的特性,但仍有一部分主动脉瓣置换术(AVR)是在紧急/急诊情况下进行的。我们试图确定紧急/急诊AVR的预测因素、结局以及预防紧急/急诊AVR的潜在机会。
我们分析了医疗保险数据,以识别2017年至2022年期间接受AVR的患者。我们使用多变量回归来确定与非选择性AVR相关的因素;我们还研究了非选择性AVR与临床结局和医疗保健成本之间的关联。
在研究期间,共有15305例患者接受了AVR(16%为紧急/急诊)。与接受择期AVR的患者相比,接受紧急/急诊AVR的患者更常为黑人或西班牙裔,尽管91.7%的患者在前一年看过心脏病专家或初级保健提供者,但他们被诊断为主动脉瓣狭窄的可能性较小。在多变量调整分析中,同时参加医疗保险和医疗补助、男性以及近期心力衰竭住院与紧急/急诊AVR风险增加相关;相反,近期主动脉瓣狭窄诊断和心脏病专家就诊与紧急/急诊AVR几率降低相关。反过来,与择期AVR相比,紧急/急诊AVR增加了住院死亡、入住重症监护病房以及出院至机构而非家中的风险,此外还延长了住院时间并增加了医疗保健成本。
紧急/急诊AVR在黑人、西班牙裔以及符合医疗保险和医疗补助双重资格的患者中更为常见。非选择性AVR还与更差的医院结局以及更高的医疗保健成本相关。重要的是,主动脉瓣狭窄诊断时间的差异似乎是一个关键决定因素;因此,加强筛查工作可能会改善结局并减少差异。