Zheng Jianqi, Yan Zeping, Wang Runchen, Xiao Houlu, Chen Zhenlin, Ge Xiaomin, Li Zhigang, Liu Zhichao, Yu Hong, Liu Hongxu, Wang Guan, Yu Pingwen, Fu Junke, Zhang Guangjian, Zhang Jia, Liu Bohao, Huang Ying, Deng Hongshen, Wang Chudong, Fu Wenhai, Zhang Yuan, Wang Rui, Jiang Yu, Lin Yuechun, Huang Linchong, Yang Chao, Cui Fei, He Jianxing, Liang Hengrui
Department of Thoracic Surgery and Oncology, the First Affiliated Hospital of Guangzhou Medical University, State Key Laboratory of Respiratory Disease, National Clinical Research Center for Respiratory Disease, Guangzhou Institute of Respiratory Health, Guangzhou, Guangdong, China.
Yuefa Health Technology (Guangzhou) Co., Ltd, Guangzhou, Guangdong, China.
J Immunother Cancer. 2025 May 31;13(5):e011773. doi: 10.1136/jitc-2025-011773.
Accurate preoperative prediction of major pathological response or pathological complete response after neoadjuvant chemo-immunotherapy remains a critical unmet need in resectable non-small-cell lung cancer (NSCLC). Conventional size-based imaging criteria offer limited reliability, while biopsy confirmation is available only post-surgery.
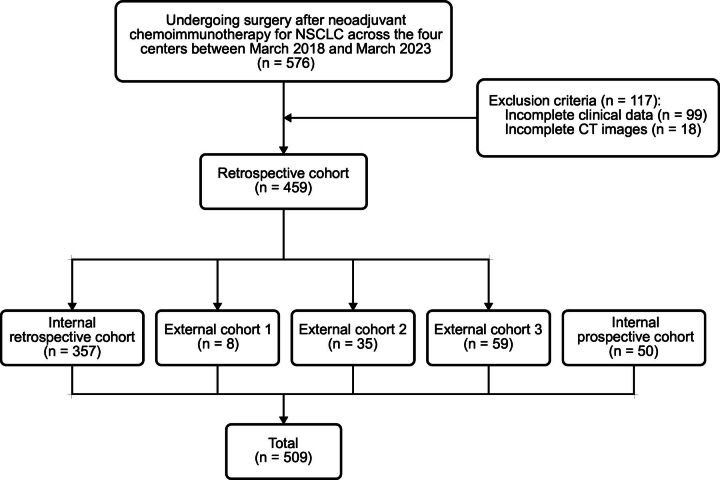
We retrospectively assembled 509 consecutive NSCLC cases from four Chinese thoracic-oncology centers (March 2018 to March 2023) and prospectively enrolled 50 additional patients. Three 3-dimensional convolutional neural networks (pre-treatment CT, pre-surgical CT, dual-phase CT) were developed; the best-performing dual-phase model (NeoPred) optionally integrated clinical variables. Model performance was measured by area under the receiver-operating-characteristic curve (AUC) and compared with nine board-certified radiologists.
In an external validation set (n=59), NeoPred achieved an AUC of 0.772 (95% CI: 0.650 to 0.895), sensitivity 0.591, specificity 0.733, and accuracy 0.627; incorporating clinical data increased the AUC to 0.787. In a prospective cohort (n=50), NeoPred reached an AUC of 0.760 (95% CI: 0.628 to 0.891), surpassing the experts' mean AUC of 0.720 (95% CI: 0.574 to 0.865). Model assistance raised the pooled expert AUC to 0.829 (95% CI: 0.707 to 0.951) and accuracy to 0.820. Marked performance persisted within radiological stable-disease subgroups (external AUC 0.742, 95% CI: 0.468 to 1.000; prospective AUC 0.833, 95% CI: 0.497 to 1.000).
Combining dual-phase CT and clinical variables, NeoPred reliably and non-invasively predicts pathological response to neoadjuvant chemo-immunotherapy in NSCLC, outperforms unaided expert assessment, and significantly enhances radiologist performance. Further multinational trials are needed to confirm generalizability and support surgical decision-making.
对于可切除的非小细胞肺癌(NSCLC),术前准确预测新辅助化疗免疫治疗后的主要病理反应或病理完全缓解仍然是一个关键的未满足需求。传统的基于大小的影像学标准可靠性有限,而活检确认仅在术后进行。
我们回顾性收集了来自四个中国胸肿瘤中心(2018年3月至2023年3月)的509例连续NSCLC病例,并前瞻性纳入了另外50例患者。开发了三个三维卷积神经网络(治疗前CT、手术前CT、双期CT);性能最佳的双期模型(NeoPred)可选择整合临床变量。通过受试者操作特征曲线下面积(AUC)来衡量模型性能,并与九名获得委员会认证的放射科医生进行比较。
在一个外部验证集(n = 59)中,NeoPred的AUC为0.772(95%CI:0.650至0.895),敏感性为0.591,特异性为0.733,准确性为0.627;纳入临床数据后,AUC提高到0.787。在一个前瞻性队列(n = 50)中,NeoPred的AUC达到0.760(95%CI:0.628至0.891),超过了专家的平均AUC 0.720(95%CI:0.574至0.865)。模型辅助将专家的合并AUC提高到0.829(95%CI:0.707至0.951),准确性提高到0.820。在放射学稳定疾病亚组中,显著的性能持续存在(外部AUC 0.742,95%CI:0.468至1.000;前瞻性AUC 0.833,95%CI:0.497至1.000)。
结合双期CT和临床变量,NeoPred能够可靠且无创地预测NSCLC新辅助化疗免疫治疗的病理反应,优于未经辅助的专家评估,并显著提高放射科医生的性能。需要进一步的多国试验来确认其普遍性并支持手术决策。