Gavelli Francesco, De Vita Nello, Lai Christopher, Azzolina Danila, Pavot Arthur, Jozwaik Mathieu, Shi Rui, Adda Imane, Beurton Alexandra, Teboul Jean-Louis, Monnet Xavier
Service de médecine intensive-réanimation, Hôpital de Bicêtre, DMU CORREVE, Université Paris-Saclay, AP-HP, Inserm UMR S_999, FHU SEPSIS, CARMAS, Le Kremlin-Bicêtre, France.
Emergency Medicine Unit, Department of Translational Medicine, Università degli Studi del Piemonte Orientale, Novara, 28100, Italy.
Crit Care. 2025 Jun 13;29(1):241. doi: 10.1186/s13054-025-05483-8.
The end-expiratory occlusion (EEO) test detects preload responsiveness through changes in cardiac index (ΔCI) during a 15-second respiratory hold at end-expiration. We investigated the diagnostic accuracy of EEO-induced changes in arterial pulse pressure (∆PP), especially when the duration of EEO is reduced to 10'' and 5'', and whether adding an end-inspiratory occlusion (EIO) improves this diagnostic accuracy.
In 143 mechanically ventilated patients with sinus rhythm, EEO and EIO were performed while recording ΔCI and ∆PP values. Either a fluid bolus-induced ΔCI ≥ 15% or a passive leg raising-induced ΔCI ≥ 10% defined preload responsiveness. The effects of the EEO and EIO tests on PP and CI were evaluated as the percentage difference between values averaged either over the last five seconds of the 15-sec respiratory holds (ΔPP and ΔPP, ΔCI and ΔCI), or between the 5th and the 10th seconds of the 15-sec respiratory holds (ΔPP and ΔPP, ΔCI and ΔCI), or during the five first seconds of respiratory holds (ΔPP and ΔPP, ΔCI and ΔCI) and baseline.
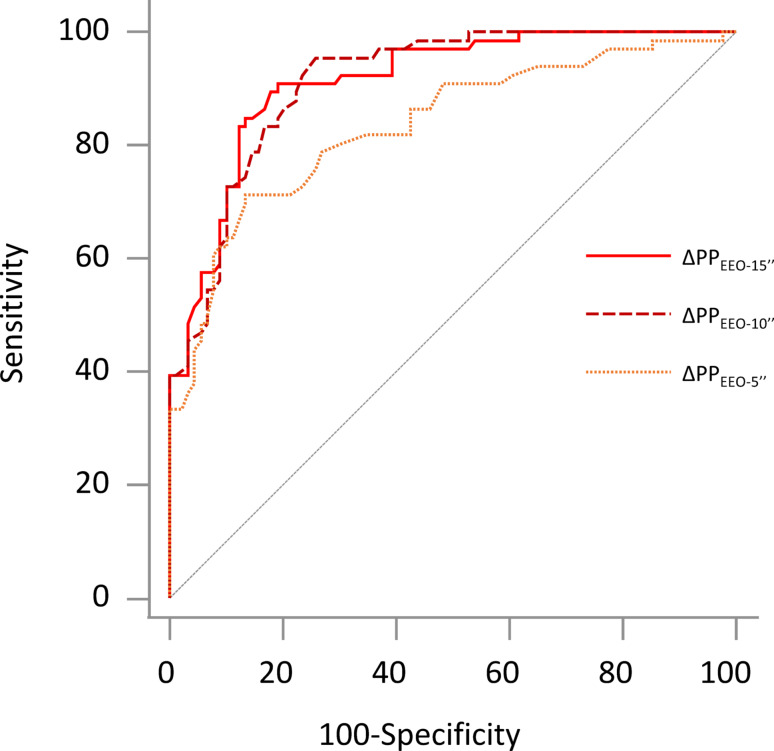
Sixty-one (43%) patients were preload responders. Both ∆CI and ∆CI were higher in responders than in non-responders (5.8 [4.5-7.3]% vs. 1.1 [0.1-3.4]% and 3.0 [2.4-4.3]% vs. 0.6 [0.1-1.6]%, respectively; p < 0.001), whereas ∆CI did not differ between responders and non-responders. ∆PP, ∆PP and ∆PP were significantly higher in responders than in non-responders (5.2 [2.8-8.7]% vs. 1.2 [0.3-2.8]%, 7.7 [5.0-12.4]% vs. 1.8 [0.5-3.1]% and 8.1 [5.1-11.8]% vs. 1.5 [0.5-3.0]%, respectively; p < 0.001). For detecting preload responsiveness, compared to the area under the receiver operating characteristic (AUROC) of ∆CI (0.935 [0.881-0.969]), the AUROC of ∆CI was similar (0.910 [0.851-0.951], p = 0.410), but the AUROC of ∆CI was smaller (0.541 [0.456-0.625], p < 0.001); the AUROC of ∆PP (0.913 [0.857-0.952], p = 0.346), and ∆PP (0.912 [0.860-0.947], p = 0.336) were similar, but the AUROC of ∆PP (0.834 (0.763-0.891, p = 0.005) was significantly smaller. Evaluation of ∆CI and ∆PP did not enhance reliability of the test at each test duration.
In ventilated patients with sinus rhythm, real-time changes in PP during a 10-second EEO reliably detect preload responsiveness.
No. IDRCB 2010A0095942. Registered 04 January 2010.
呼气末阻断(EEO)试验通过在呼气末屏气15秒期间心脏指数(ΔCI)的变化来检测前负荷反应性。我们研究了EEO引起的动脉脉压变化(∆PP)的诊断准确性,特别是当EEO持续时间缩短至10秒和5秒时,以及增加吸气末阻断(EIO)是否能提高这种诊断准确性。
对143例窦性心律的机械通气患者进行EEO和EIO,同时记录ΔCI和∆PP值。液体负荷诱导的ΔCI≥15%或被动抬腿诱导的ΔCI≥10%定义为前负荷反应性。EEO和EIO试验对PP和CI的影响评估为15秒屏气的最后五秒(ΔPP和ΔPP,ΔCI和ΔCI)、15秒屏气的第5秒和第10秒(ΔPP和ΔPP,ΔCI和ΔCI)或屏气的前五秒(ΔPP和ΔPP,ΔCI和ΔCI)与基线值的平均百分比差异。
61例(43%)患者为前负荷反应者。反应者的∆CI和ΔCI均高于无反应者(分别为5.8 [4.5 - 7.3]%对1.1 [0.1 - 3.4]%和3.0 [2.4 - 4.3]%对0.6 [0.1 - 1.6]%;p < 0.001),而反应者与无反应者之间的ΔCI无差异。反应者的∆PP、ΔPP和ΔPP显著高于无反应者(分别为5.2 [2.8 - 8.7]%对1.2 [0.3 - 2.8]%、7.7 [5.0 - 12.4]%对1.8 [0.5 - 3.1]%和8.1 [5.1 - 11.8]%对1.5 [0.5 - 3.0]%;p < 0.001)。对于检测前负荷反应性,与ΔCI的受试者工作特征曲线下面积(AUROC)(0.935 [0.881 - 0.969])相比,ΔCI的AUROC相似(0.910 [0.851 - 0.951],p = 0.410),但ΔCI的AUROC较小(0.541 [0.456 - 0.625],p < 0.001);∆PP的AUROC(0.913 [0.857 - 0.952],p = 0.346)和ΔPP的AUROC(0.912 [0.860 - 0.947],p = 0.336)相似,但ΔPP的AUROC(0.834 [0.763 - 0.891],p = 0.005)显著较小。在每个试验持续时间评估ΔCI和∆PP并未提高试验的可靠性。
在窦性心律的机械通气患者中,10秒EEO期间PP的实时变化可可靠地检测前负荷反应性。
编号IDRCB 2010A0095942。2010年1月4日注册。