Zhu Yun, Zhang Shuni, Wei Wei, Yang Li, Wang Lingling, Wang Ying, Fan Ye, Sun Haitao, Xie Zongyu
Department of Radiology, The First Affiliated Hospital of Bengbu Medical University, Bengbu, Anhui, China.
Department of Radiology, Anhui No.2 Provincial People's Hospital, Hefei, China.
Front Oncol. 2025 Jun 4;15:1561599. doi: 10.3389/fonc.2025.1561599. eCollection 2025.
This study aimed to create a nomogram model (NM) that combines clinical-radiological factors with radiomics features of both intra- and peritumoral regions extracted from pretherapy dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) images, in order to establish a reliable method for early prediction of pathological complete response (pCR) to neoadjuvant chemotherapy (NAC) in patients with breast cancer.
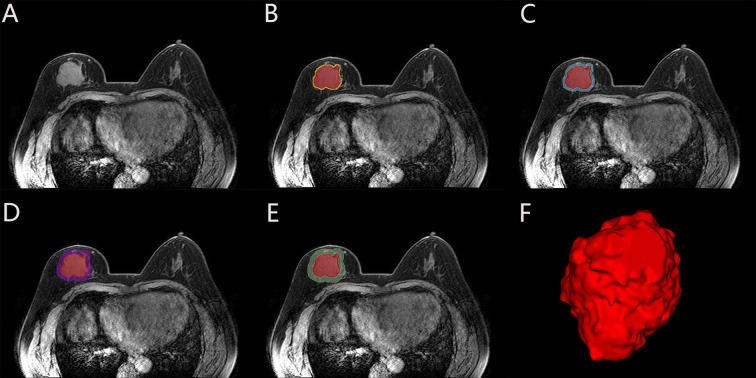
A total of 214 patients were randomly divided into a training set (n=149) and a test set (n=65) in a ratio of 7:3. Radiomics features were extracted from intratumoral region and 2-mm, 4-mm, 6-mm, 8-mm peritumoral regions on DCE-MRI images, and selected the optimal peritumoral region. The intratumoral radiomics model (IRM), 2-mm, 4-mm, 6-mm, 8-mm peritumoral radiomics model (PRM), the combined intra- and the optimal peritumoral radiomics model (CIPRM) were constructed based on five machine learning algorithms, and then the radiomics scores (Rad-score) were obtained. Independent risk factors for clinical-radiological features were obtained by univariate and multivariate logistic regression analysis, and clinical model (CM) was constructed. Finally, the CIPRM Rad-score combined with clinical-radiological factors was used to construct a NM. The performance of different models were evaluated by receiver operating characteristic curve (ROC) analysis, calibration curve analysis, and decision curve analysis (DCA).
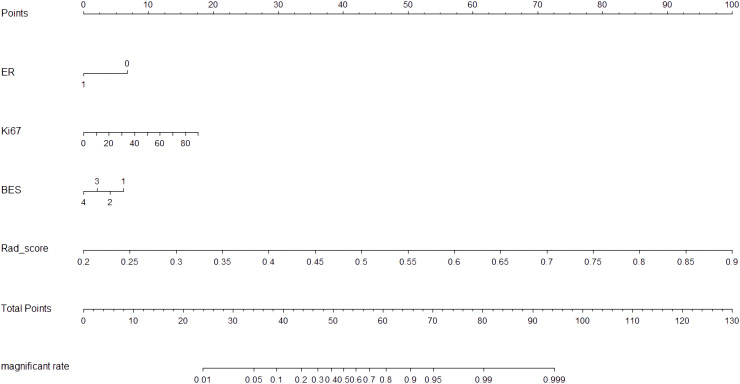
In our study, the 6-mm peritumoral size was considered to be the optimal peritumoral region. The CM is constructed based on three independent risk factors: estrogen receptor (ER), Ki-67, and breast edema score (BES). Incorporating ER, Ki-67, BES, and CIPRM Rad-score (combined intra- and 6-mm peritumoral) into the nomogram achieved a reliable predictive performance. And the area under the curve (AUC), sensitivity, specificity, and accuracy of the NM was 0.911, 0.848, 0.831, 0.826 for the training set and 0.897, 0.893, 0.784, 0.815 for the test set, respectively.
The NM has a good value for early prediction of pCR after NAC in breast cancer patients.
本研究旨在创建一种列线图模型(NM),该模型将临床放射学因素与从治疗前动态对比增强磁共振成像(DCE-MRI)图像中提取的肿瘤内和瘤周区域的放射组学特征相结合,以建立一种可靠的方法来早期预测乳腺癌患者新辅助化疗(NAC)后的病理完全缓解(pCR)。
总共214例患者以7:3的比例随机分为训练集(n = 149)和测试集(n = 65)。从DCE-MRI图像上的肿瘤内区域以及瘤周2毫米、4毫米、6毫米、8毫米区域提取放射组学特征,并选择最佳瘤周区域。基于五种机器学习算法构建肿瘤内放射组学模型(IRM)、2毫米、4毫米、6毫米、8毫米瘤周放射组学模型(PRM)、肿瘤内与最佳瘤周联合放射组学模型(CIPRM),然后获得放射组学评分(Rad-score)。通过单因素和多因素逻辑回归分析获得临床放射学特征的独立危险因素,并构建临床模型(CM)。最后,将CIPRM Rad-score与临床放射学因素相结合构建NM。通过受试者工作特征曲线(ROC)分析、校准曲线分析和决策曲线分析(DCA)评估不同模型的性能。
在我们的研究中,6毫米的瘤周大小被认为是最佳瘤周区域。CM基于三个独立危险因素构建:雌激素受体(ER)、Ki-67和乳腺水肿评分(BES)。将ER、Ki-67、BES和CIPRM Rad-score(肿瘤内与6毫米瘤周联合)纳入列线图可实现可靠的预测性能。训练集的列线图曲线下面积(AUC)、敏感性、特异性和准确性分别为0.911、0.848、0.831、0.826,测试集分别为0.897、0.893、0.784、0.815。
该列线图对乳腺癌患者NAC后pCR的早期预测具有良好价值。