Frank Daniel, Forst Anna, Ortmann Christopher, Gehring Stephan, König Tatjana T, Wittenmeier Eva
Department of Anesthesiology, University Medical Centre Mainz, Johannes Gutenberg University, 55131 Mainz, Germany.
Children's Hospital, University Medical Centre Mainz, Johannes Gutenberg University, 55131 Mainz, Germany.
J Clin Med. 2025 Jun 9;14(12):4063. doi: 10.3390/jcm14124063.
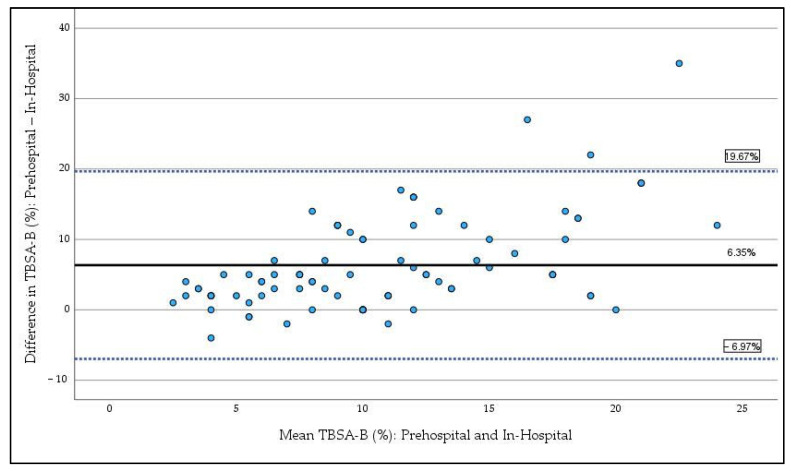
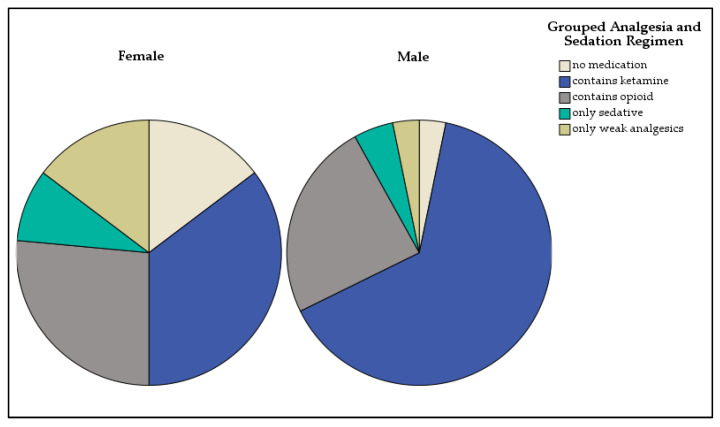
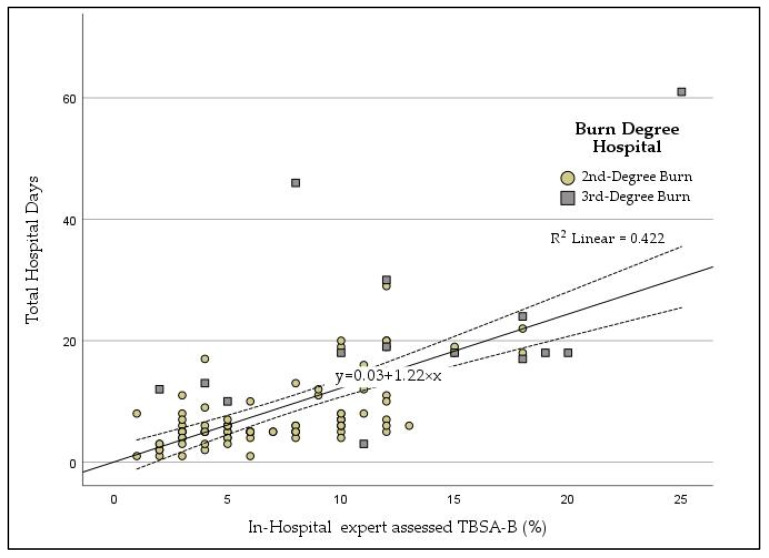
Accurate prehospital assessment of total body surface area burned (TBSA-B) is crucial for pediatric burn management, guiding resuscitation, fluid therapy, and transfer decisions. This study evaluates the accuracy of prehospital TBSA-B estimations compared to in-hospital expert assessment and examines their impact on prehospital management. This retrospective study analyzed 104 pediatric burn cases (median 17 months; 5 days-14 years) from 2017 to 2021. The primary endpoint was the difference between prehospital TBSA-B estimation and clinical measurement, with a clinically significant discrepancy defined as >5%. Secondary endpoints included the relationship between TBSA-B estimation and fluid therapy, analgesia, and hospital stay duration. Prehospital TBSA-B estimations ranged from 2% to 40% (mean: 13.9%, SD = 4.4%) with scalds being the most common burn type (90.4%). Bland-Altman analysis showed a mean TBSA-B overestimation (bias) of 6.35%, with limits of agreement ranging from -6.97% (CI: -9.42 to -4.51) to 19.67% (CI: 17.21 to 22.12). No significant patterns in overestimation were associated with age, gender, or burn location. Fluid therapy volumes were independent of prehospital TBSA-B estimates, and analgesic administration varied by gender, with girls receiving less analgesia than boys, but showed no association with burn extent or severity. Hospital stay duration correlated proportionally with in-hospital assessed TBSA-B. Prehospital TBSA-B estimation was systematically overestimated, yet it did not influence fluid therapy decisions. Gender differences were observed in analgesic administration, while hospital stay duration was directly related to burn extent. These findings highlight the need for improved training and standardized tools to enhance prehospital burn assessment in pediatric patients.
准确的院前烧伤总面积(TBSA-B)评估对于小儿烧伤治疗至关重要,可指导复苏、液体治疗及转运决策。本研究评估了院前TBSA-B估计值与院内专家评估相比的准确性,并探讨其对院前管理的影响。这项回顾性研究分析了2017年至2021年期间的104例小儿烧伤病例(中位年龄17个月;5天至14岁)。主要终点是院前TBSA-B估计值与临床测量值之间的差异,临床显著差异定义为>5%。次要终点包括TBSA-B估计值与液体治疗、镇痛及住院时间之间的关系。院前TBSA-B估计值范围为2%至40%(平均:13.9%,标准差 = 4.4%),烫伤是最常见的烧伤类型(90.4%)。Bland-Altman分析显示,TBSA-B平均高估(偏差)6.35%,一致性界限范围为-6.97%(CI:-9.42至-4.51)至19.67%(CI:17.21至22.12)。高估情况与年龄、性别或烧伤部位无显著关联。液体治疗量与院前TBSA-B估计值无关,镇痛药物的使用因性别而异,女孩接受的镇痛药物比男孩少,但与烧伤程度或严重程度无关。住院时间与院内评估的TBSA-B成比例相关。院前TBSA-B估计值存在系统性高估,但并未影响液体治疗决策。在镇痛药物使用方面观察到性别差异,而住院时间与烧伤程度直接相关。这些发现凸显了改进培训和标准化工具以加强小儿患者院前烧伤评估的必要性。