Babu Eldo, Ghosh Parvathy, Sarika K, James Anju, Sapna Varma N K, Ajith V V
Department of Orthodontics & Dentofacial Orthopedics, Amrita School of Dentistry, Amrita Vishwa Vidyapeetham, Kochi, Kerala, India.
Department of Public Health Dentistry, Amrita School of Dentistry, Amrita Vishwa Vidyapeetham, Kochi, Kerala, India.
J Oral Biol Craniofac Res. 2025 Jul-Aug;15(4):837-848. doi: 10.1016/j.jobcr.2025.06.001. Epub 2025 Jun 11.
Le-Fort I osteotomy is commonly performed in cleft lip and palate patients to correct maxillary discrepancies, potentially influencing pharyngeal airway dimensions and velopharyngeal function. Thus, the review aims to evaluate the effects on pharyngeal airway and velopharyngeal function following Le-Fort I osteotomy in cleft lip and palate patients.
This systematic review followed the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA). A comprehensive electronic search in databases of Scopus, EBSCO, PubMed, Cochrane, CINAHL, ScienceDirect and Google Scholar was performed to identify studies published from inception to August 2024 with language restricted to English. The critical appraisal using NIH quality assessment tool and data extraction processes were carried out independently by two reviewers. A meta-analysis was conducted to determine the effects of Le-Fort I on nasopharyngeal, oropharyngeal and hypopharyngeal airway depth before and after the intervention. Quality was evaluated using GRADE.
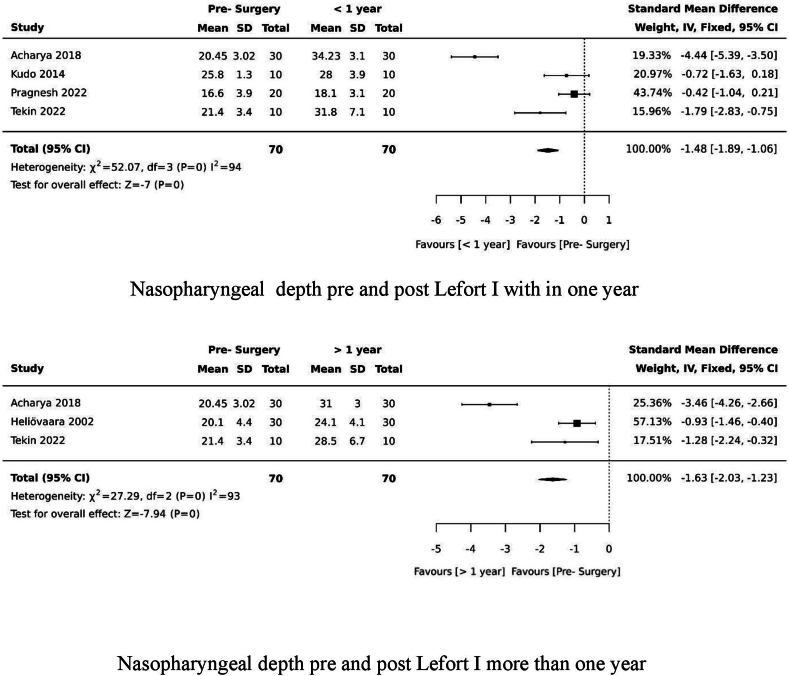
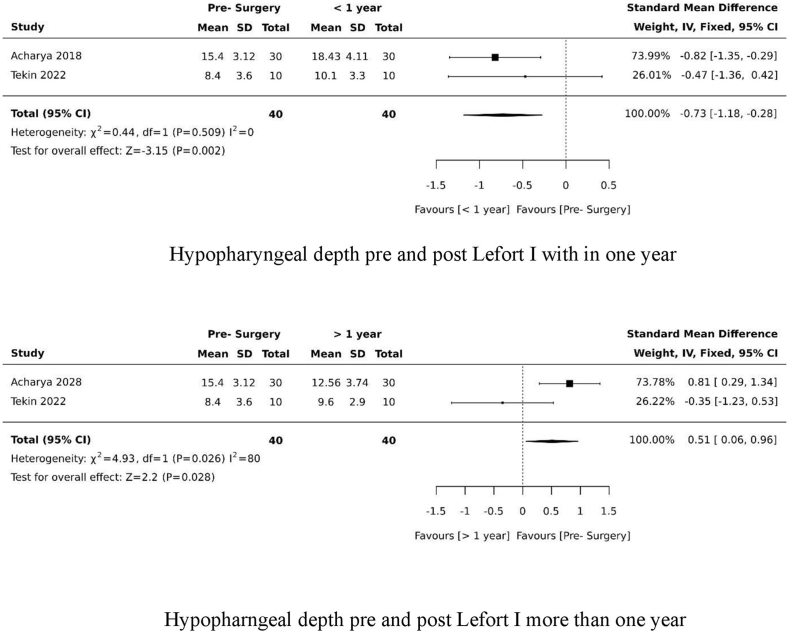
Twelve articles were included in this review. Le-Fort I maxillary advancement significantly increases pharyngeal airway dimensions, particularly in the nasopharyngeal and oropharyngeal regions, with most studies reporting improved airway space postoperatively. However, velopharyngeal function outcomes were variable: some patients experienced transient increases in nasalance or hypernasality, while others showed no significant adverse effects. Notably, preoperative hypernasality may predict postoperative velopharyngeal insufficiency.
Le-Fort I maxillary advancement increases pharyngeal airway volume; particularly in the nasopharyngeal and oropharyngeal regions; thereby improving breathing function, especially during sleep. However, the degree of airway expansion varies depending on the extent of surgery and preoperative airway conditions. While the procedure often enhances velopharyngeal closure by improving anatomical alignment and muscle coordination, it also carries a risk of worsening velopharyngeal insufficiency if the maxilla is advanced beyond a certain limit, which differs among individuals.
唇腭裂患者常进行勒福Ⅰ型截骨术以矫正上颌骨差异,这可能会影响咽气道尺寸和腭咽功能。因此,本综述旨在评估唇腭裂患者接受勒福Ⅰ型截骨术后对咽气道和腭咽功能的影响。
本系统综述遵循系统评价和Meta分析的首选报告项目(PRISMA)中概述的指南。在Scopus、EBSCO、PubMed、Cochrane、CINAHL、ScienceDirect和谷歌学术等数据库中进行全面的电子检索,以识别从创刊至2024年8月发表的研究,语言限制为英语。由两名 reviewers 独立进行使用美国国立卫生研究院质量评估工具的批判性评价和数据提取过程。进行Meta分析以确定干预前后勒福Ⅰ型截骨术对鼻咽、口咽和下咽气道深度的影响。使用GRADE评估质量。
本综述纳入了12篇文章。勒福Ⅰ型上颌骨前移显著增加咽气道尺寸,尤其是在鼻咽和口咽区域,大多数研究报告术后气道空间有所改善。然而,腭咽功能的结果各不相同:一些患者鼻音或高鼻音出现短暂增加,而另一些患者则未显示出明显的不良影响。值得注意的是,术前高鼻音可能预示术后腭咽闭合不全。
勒福Ⅰ型上颌骨前移增加咽气道容积;尤其是在鼻咽和口咽区域;从而改善呼吸功能,尤其是在睡眠期间。然而,气道扩张的程度因手术范围和术前气道状况而异。虽然该手术通常通过改善解剖结构对齐和肌肉协调来增强腭咽闭合,但如果上颌骨前移超过一定限度,也有导致腭咽闭合不全恶化的风险,且个体之间存在差异。