Tian Tu-Lei, Wu Guan-Wei, Xie Mei-Ling, Qu Xiang-Kun, Wang Xiao-Tong, Sun Chang-Lu
Department of Respiratory and Critical Care Medicine, The Affiliated Bozhou Hospital of Anhui Medical University, Bozhou, Anhui, China.
Department of Urology, Affiliated Wuhu Hospital of East China Normal University, Wuhu, Anhui, China.
Front Med (Lausanne). 2025 Jun 13;12:1553188. doi: 10.3389/fmed.2025.1553188. eCollection 2025.
The lymphocyte-to-high-density lipoprotein ratio (LHR), a novel biomarker reflecting systemic inflammation and immune status, has been widely studied in various diseases. However, its association with mortality risk among asthma patients remains unexplored.
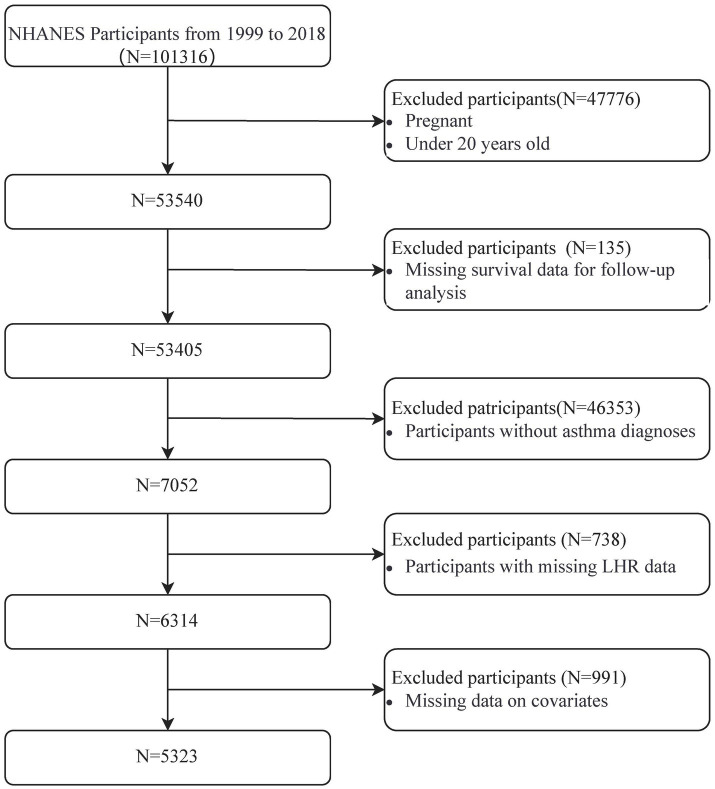
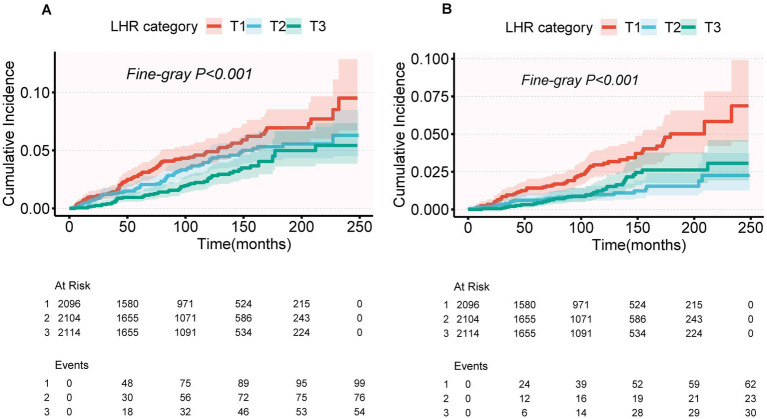
This study utilized data from the National Health and Nutrition Examination Survey (NHANES) spanning 1999-2018, including 5,323 adult asthma patients. Mortality outcomes were ascertained through linkage with the National Death Index (NDI) up to December 31, 2019. Cox proportional hazards models and Fine-Gray competing risk models were employed to examine the association between LHR and mortality risks. Dose-response relationships were assessed using restricted cubic spline analyses.
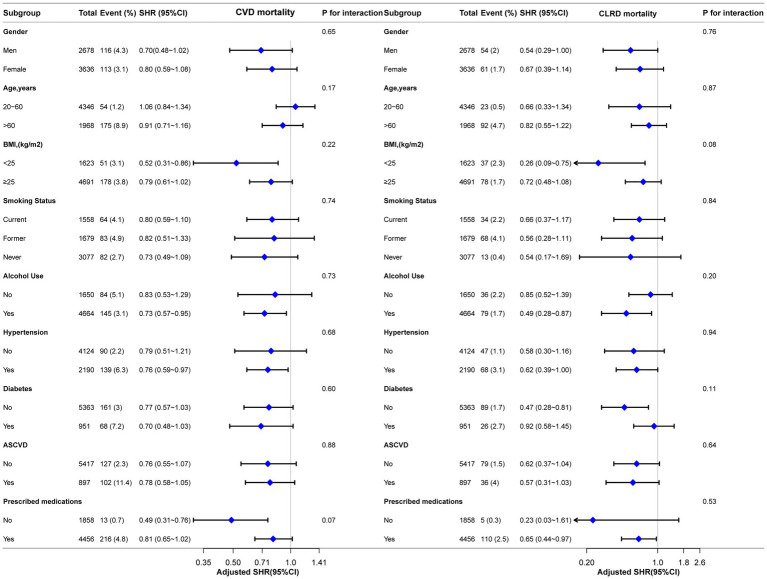
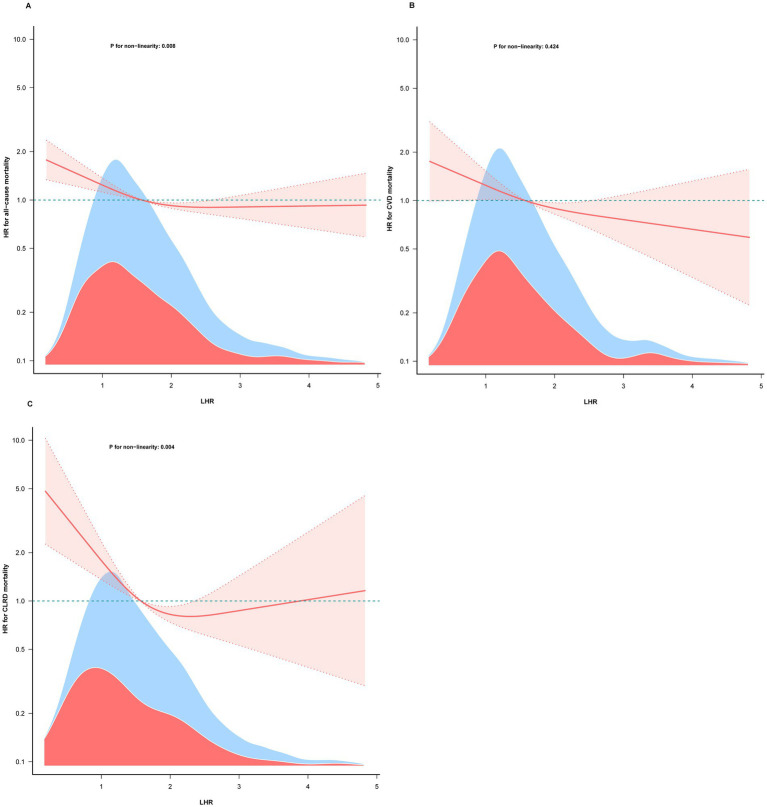
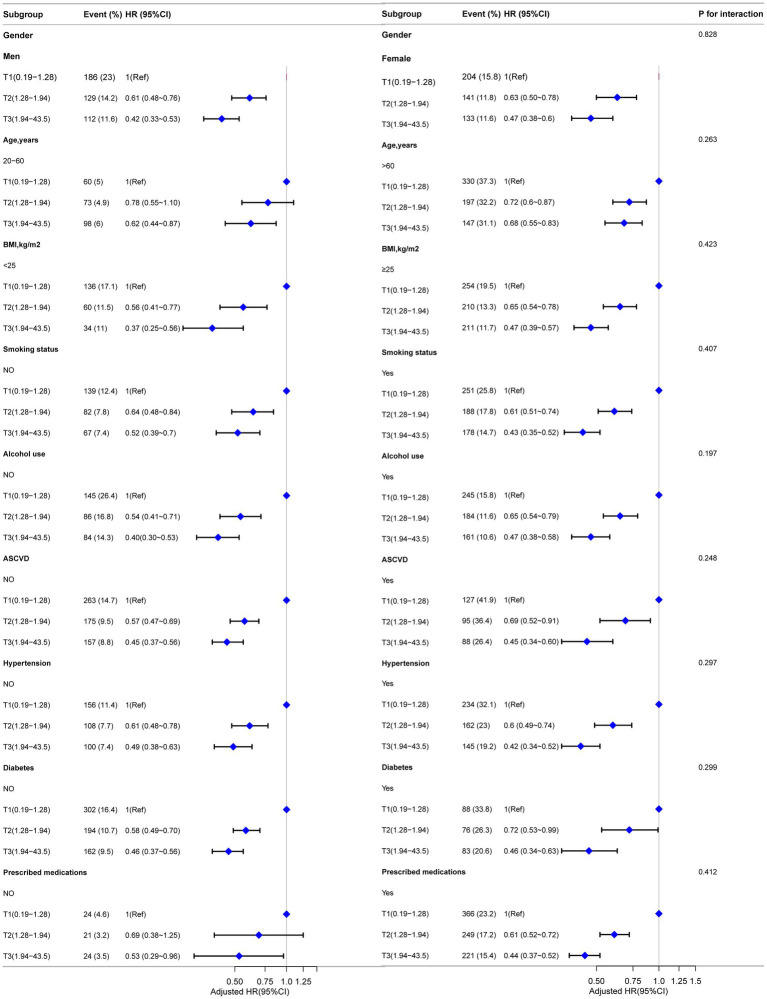
Over a mean follow-up period of 106.95 months, 724 all-cause deaths (13.6%) were recorded. After multivariable adjustment, a one-unit increase in log-transformed LHR was associated with reduced risks of mortality: 18% for all-cause (HR = 0.82, 95% CI: 0.74-0.91), 21% for cardiovascular disease (CVD) (HR = 0.79, 95% CI: 0.65-0.96), and 41% for chronic lower respiratory disease (CLRD) (HR = 0.59, 95% CI: 0.45-0.77). Restricted cubic spline analyses showed an L-shaped association of LHR with all-cause and CLRD mortality, with inflection points at 1.78 and 1.52, respectively. For CVD mortality, a linear association was observed. Competing risk models further confirmed the association of LHR with reduced CLRD mortality (SHR = 0.64, 95% CI: 0.46-0.88), while the association with CVD mortality was no longer significant (SHR = 0.85, 95% CI: 0.70-1.03).
LHR is nonlinearly associated with all-cause and CLRD mortality and shows a significant inverse association with CLRD mortality risk. These findings were further validated using competing risk models, highlighting the robustness of the results.
淋巴细胞与高密度脂蛋白比值(LHR)是一种反映全身炎症和免疫状态的新型生物标志物,已在多种疾病中得到广泛研究。然而,其与哮喘患者死亡风险的关联仍未得到探索。
本研究利用了1999年至2018年美国国家健康与营养检查调查(NHANES)的数据,其中包括5323名成年哮喘患者。通过与截至2019年12月31日的国家死亡指数(NDI)进行关联来确定死亡结局。采用Cox比例风险模型和Fine-Gray竞争风险模型来检验LHR与死亡风险之间的关联。使用受限立方样条分析评估剂量反应关系。
在平均106.95个月的随访期内,记录了724例全因死亡(13.6%)。经过多变量调整后,对数转换后的LHR每增加一个单位,与死亡风险降低相关:全因死亡风险降低18%(HR = 0.82,95%CI:0.74 - 0.91),心血管疾病(CVD)死亡风险降低21%(HR = 0.79,95%CI:0.65 - 0.96),慢性下呼吸道疾病(CLRD)死亡风险降低41%(HR = 0.59,95%CI:0.45 - 0.77)。受限立方样条分析显示LHR与全因和CLRD死亡率呈L形关联,拐点分别为1.78和1.52。对于CVD死亡率,观察到呈线性关联。竞争风险模型进一步证实了LHR与CLRD死亡率降低之间的关联(SHR = 0.64,95%CI:0.46 - 0.88),而与CVD死亡率的关联不再显著(SHR = 0.85,95%CI:0.70 - 1.03)。
LHR与全因和CLRD死亡率呈非线性关联,并与CLRD死亡风险呈显著负相关。使用竞争风险模型进一步验证了这些发现,突出了结果的稳健性。