Conley Marguerite M, Mayr Hannah L, Hepburn Kirsten S, Holland Justin J, Mudge David W, Tonges Tammy J, Modderman Richard S, Gerzina Sally A, Johnson David W, Viecelli Andrea K, MacLaughlin Helen L
School of Exercise and Nutrition Sciences, Queensland University of Technology, Brisbane, Queensland, Australia.
Department of Nutrition and Dietetics, Princess Alexandra Hospital, Brisbane, Queensland, Australia.
Kidney Int Rep. 2025 Apr 21;10(7):2153-2164. doi: 10.1016/j.ekir.2025.04.021. eCollection 2025 Jul.
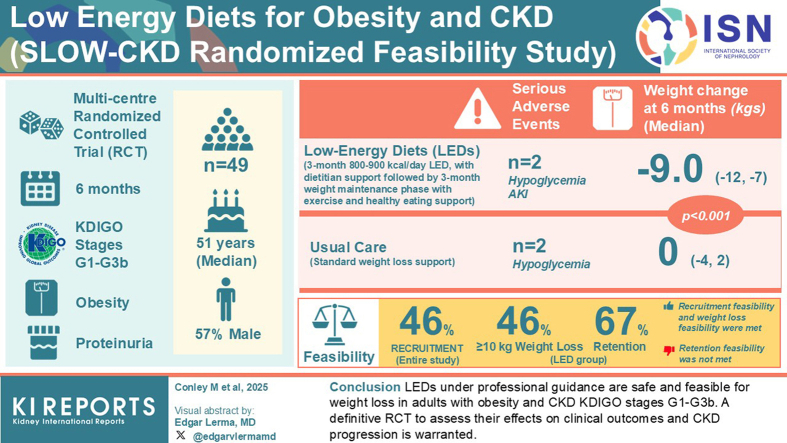
Low energy diets (LEDs) may slow disease progression; however, their effects are under researched in chronic kidney disease (CKD). This study evaluated the safety and feasibility of an LED weight management program in adults with obesity and CKD.
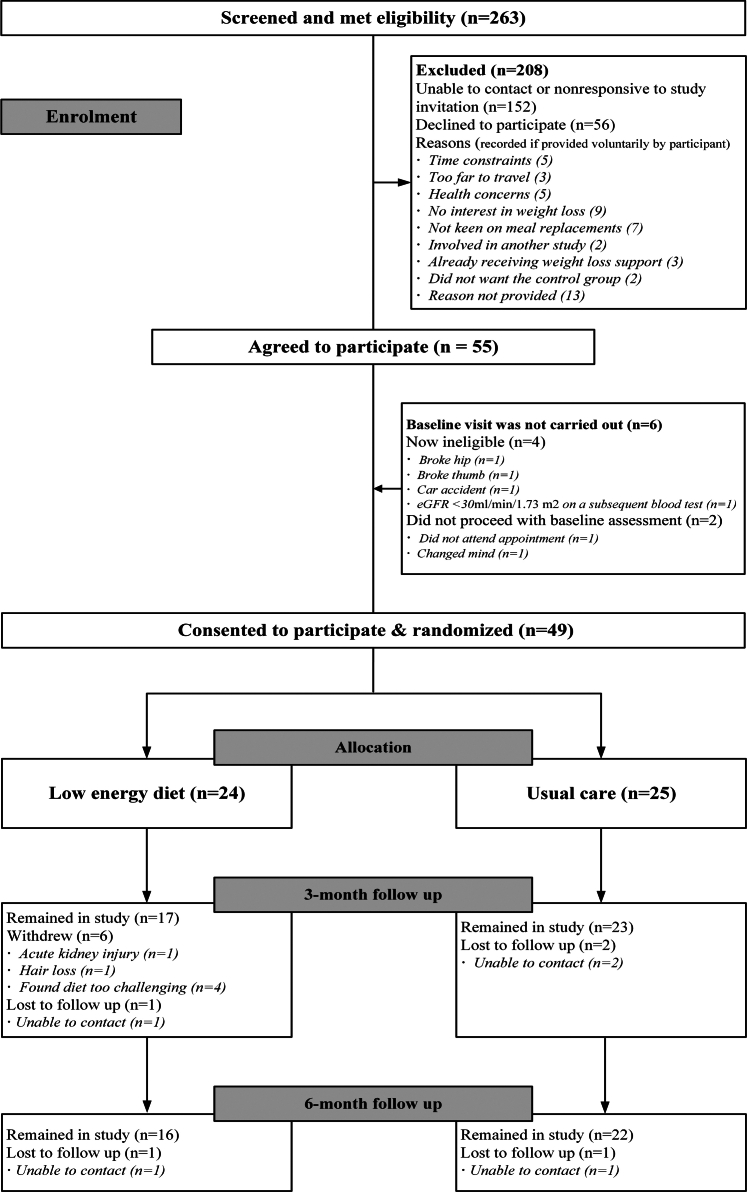
This multicenter 6-month randomized controlled trial (RCT) involved adults with CKD Kidney Disease: Improving Global Outcomes stages G1 to G3b, obesity, and proteinuria, randomized 1:1 into 2 groups. The LED group followed a 3-month 800 to 900 kcal/d LED, with dietitian support, then a 3-month weight maintenance phase with exercise and healthy eating support. The usual care (UC) group received standard clinic weight loss support. Primary outcomes were safety (serious adverse events [SAEs]) and feasibility (≥2 of recruitment rate ≥ 25%, LED group retention rate ≥ 75%, and ≥ 30% of LED group achieving ≥ 10 kg weight loss at 3 months). Secondary outcomes included changes in anthropometry, clinical measures, patient-reported outcomes, and participant experiences.
Forty-nine participants (median age 51 years, 57% male) consented. SAEs were low and comparable as follows: 2 in the LED group (hypoglycemia and acute kidney injury) and 2 in the UC group (hypoglycemia), all requiring hospitalization. Feasibility was met for recruitment (46%) and weight loss (46% achieved ≥ 10 kg loss) but not for retention (67% retained). At 6 months, median (IQR) weight change was -9.0 kg (-12 to -7) in the LED group and 0 kg (-4 to 2) in the UC group ( < 0.001).
LEDs under professional guidance are safe and feasible for weight loss in adults with obesity and CKD Kidney Disease: Improving Global Outcomes stages G1 to G3b. A definitive RCT to assess their effects on clinical outcomes and CKD progression is warranted.
低能量饮食(LEDs)可能会减缓疾病进展;然而,其在慢性肾脏病(CKD)中的作用尚未得到充分研究。本研究评估了LED体重管理计划在肥胖且患有CKD的成年人中的安全性和可行性。
这项多中心6个月随机对照试验(RCT)纳入了患有CKD(改善全球肾脏病预后组织分期为G1至G3b)、肥胖且有蛋白尿的成年人,按1:1随机分为两组。LED组在营养师的支持下遵循为期3个月、每日800至900千卡的LED饮食,然后进入为期3个月的体重维持阶段,期间给予运动和健康饮食支持。常规护理(UC)组接受标准的门诊体重减轻支持。主要结局指标为安全性(严重不良事件[SAEs])和可行性(招募率≥25%、LED组保留率≥75%以及LED组3个月时≥30%的患者体重减轻≥10千克这三项指标中至少两项达标)。次要结局指标包括人体测量学指标、临床指标、患者报告结局以及参与者体验的变化。
49名参与者(中位年龄51岁,57%为男性)同意参与研究。SAEs发生率较低且两组相当,具体如下:LED组2例(低血糖和急性肾损伤),UC组2例(低血糖),所有事件均需住院治疗。在招募(46%)和体重减轻(46%的患者体重减轻≥10千克)方面达到了可行性标准,但在保留率(67%)方面未达标。6个月时,LED组的中位(四分位间距)体重变化为-9.0千克(-12至-7),UC组为0千克(-4至2)(P<0.001)。
在专业指导下,LED饮食对于肥胖且患有CKD(改善全球肾脏病预后组织分期为G1至G3b)的成年人来说,是安全且可行的减肥方法。有必要进行一项确定性RCT来评估其对临床结局和CKD进展的影响。