Fan Qinghong, Tang Guofang, Jiang Mengling, Xu Yujuan, Pan Nenglang, Liang Zhiwei, Zhang Chuyu, Li Pinghong, Xu Feilong, Chen Zhimin, Liu Bo, Chen Lingzhen, Li Youxia, Li Chuo, Hu Fengyu, Li Feng
Institute of Infectious Diseases, Guangzhou Eighth People's Hospital, Guangzhou Medical University, Guangzhou 510440, China.
Guangzhou Key Laboratory of Clinical Pathogen Research for Infectious Diseases, Guangzhou 510440, China.
Biosaf Health. 2025 May 16;7(3):173-182. doi: 10.1016/j.bsheal.2025.05.006. eCollection 2025 Jun.
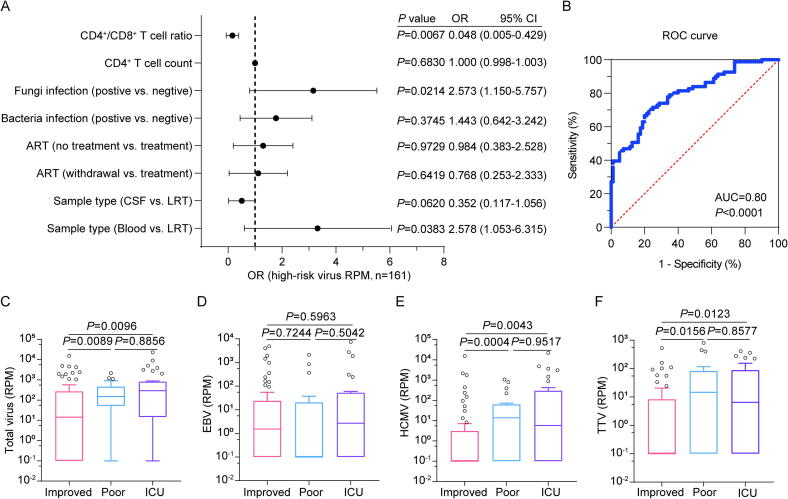
Opportunistic infections caused by viruses, bacteria, fungi, and parasites, are commonly reported in hospitalized human immunodeficiency virus (HIV)-positive patients, but their detrimental contribution to disease severity remains under explored. In this study, we examined the coinfection profiles of 126 HIV-positive patients with suspected respiratory, bloodstream, or neurological infections. Lower respiratory tract (LRT) samples, cerebrospinal fluid, and blood samples collected within the first seven days of admission were subjected to metagenomic next-generation sequencing (mNGS). Additionally, a multiplex polymerase chain reaction (PCR) detection kit to identify ten commonly known respiratory pathogens was applied to the LRT samples. Of 126 HIV-positive patients, 111 (88.1 %) were coinfected with at least one known virus. Epstein-Barr virus (EBV) (71/111, 64.0 %), human cytomegalovirus (HCMV) (64/111, 57.7 %), and torque teno virus (TTV) (63/111, 56.8 %) were the three most prevalent coinfected viruses. Fungal coinfections (58/126, 46.0 %) and bacterial coinfections (47/126, 37.3 %) were less frequent than viral coinfections. Higher viral loads of coinfection were associated with fungal coinfections (odds ratio [OR] = 2.573, 95 % confidence interval [CI]: 1.150-5.757, = 0.0214) and lower CD4/CD8 T cell ratios (OR = 0.048, 95 % CI: 0.005-0.429, = 0.0067). Importantly, patients with higher loads of HCMV and TTV, but not EBV, exhibited worse clinical outcomes. Specifically, patients with HCMV reads per million (RPM) > 0 and TTV RPM > 5 exhibited significantly higher risks of poor prognosis and intensive care unit (ICU) admission. In contrast, EBV RPM showed no association with clinical outcomes in this context. In conclusion, HCMV and TTV may serve as prognostic biomarkers linked to poorer outcomes in HIV-positive patients. Detection of HCMV and TTV could predict clinical outcomes and improve patient management strategies.
病毒、细菌、真菌和寄生虫引起的机会性感染在住院的人类免疫缺陷病毒(HIV)阳性患者中很常见,但它们对疾病严重程度的有害影响仍有待探索。在本研究中,我们检查了126例疑似呼吸道、血流或神经系统感染的HIV阳性患者的合并感染情况。对入院后前7天内采集的下呼吸道(LRT)样本、脑脊液和血液样本进行宏基因组下一代测序(mNGS)。此外,将一种用于鉴定十种常见呼吸道病原体的多重聚合酶链反应(PCR)检测试剂盒应用于LRT样本。在126例HIV阳性患者中,111例(88.1%)至少合并感染一种已知病毒。爱泼斯坦-巴尔病毒(EBV)(71/111,64.0%)、人巨细胞病毒(HCMV)(64/111,57.7%)和细小病毒B19(TTV)(63/111,56.8%)是三种最常见的合并感染病毒。真菌合并感染(58/126,46.0%)和细菌合并感染(47/126,37.3%)比病毒合并感染少见。合并感染的病毒载量较高与真菌合并感染相关(优势比[OR]=2.573,95%置信区间[CI]:1.150-5.757,P=0.0214)以及较低的CD4/CD8 T细胞比值相关(OR=0.048,95%CI:0.005-0.429,P=0.0067)。重要的是,HCMV和TTV载量较高(而非EBV)的患者临床结局较差。具体而言,每百万HCMV读数(RPM)>0且TTV RPM>5的患者预后不良和入住重症监护病房(ICU)的风险显著更高。相比之下,在这种情况下EBV RPM与临床结局无关。总之,HCMV和TTV可能作为与HIV阳性患者较差结局相关的预后生物标志物。检测HCMV和TTV可以预测临床结局并改善患者管理策略。