Palasamudram Shekar Saketh, Sivasubramanian Barath Prashanth, Ravikumar Diviya Bharathi, Qadeer Husna, Ismail Sharieff Ibthisam, Prasad Rhea, Chandra Pokhriyal Sindhu, Bellamkonda Amulya, Balla Mamtha, Dalal Rutul
Interventional Pulmonology, Pulmonary and Sleep Associates of Huntsville, Huntsville, USA.
Internal Medicine, Northeast Georgia Medical Center, Gainesville, USA.
Cureus. 2025 Jun 22;17(6):e86534. doi: 10.7759/cureus.86534. eCollection 2025 Jun.
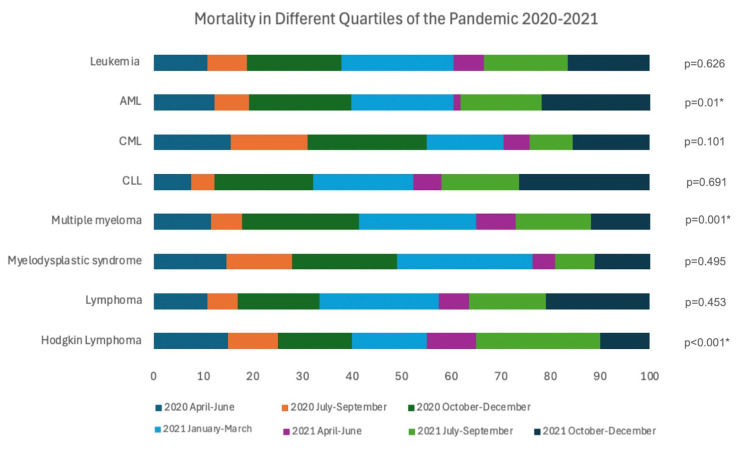
Background Patients with hematological malignancies face a substantially increased mortality from COVID-19. Although the peak of the COVID-19 pandemic has passed, the virus remains common, and understanding its impact on vulnerable groups such as those with hematologic malignancies remains crucial. Limited research exists on mortality patterns in leukemia and lymphoma patients during the pandemic. Studying these outcomes provides important insights into how different waves of COVID-19 affected immunocompromised individuals and supports the development of strategies for prevention, patient care, and risk reduction, which are essential both for managing emerging variants and preventing future pandemics. We aimed to identify the mortality risk of COVID-19 in leukemia (LekCov-19) and lymphoma (LymCov-19) in the United States and the mortality trends between each quartile from 2020 to 2021. Methods We analyzed the National Inpatient Sample database (2020-2021) to include adults (≥18 years) having leukemia and lymphoma admitted for COVID-19. Descriptive analysis, propensity matching, and multivariate regression were performed, with the p-value at ≤0.05 considered statistically significant. The risk of mortality was compared between each outcome. Results Among 8,191 LekCov-19 patients, 1,200 (14.7%) experienced mortality, whereas 507 out of 2,578 LymCov-19 patients (19.7%) experienced mortality. Multivariate regression showed a two-fold increase in mortality among LekCOV-19 and LymCOV-19 (p < 0.001). In both cohorts, several organ dysfunctions, including pulmonary, renal, and cardiac dysfunctions, were associated with increased mortality (p ≤ 0.0001). Similarly, in both cohorts, signs of bone marrow dysfunction, such as pancytopenia and thrombocytopenia, showed increased odds of mortality (p < 0.01). Both cohorts exhibited varying mortality trends, peaking during October-December 2020, January-March, July-September, and October-December 2021 (p ≤ 0.01). Hematopoietic stem cell transplantation recipients had lower odds of mortality in both cohorts, but did not attain statistical significance (p > 0.05). Conclusion COVID-19 was associated with increased mortality in leukemia and lymphoma patients. Surges in COVID-19-related mortality were identified from October 2020 to March 2021, and these trends could be pivotal in forecasting future mortality risks in cancer patients. Clinicians should refine treatment regimens and prioritize advancing clinical trials to address the effects of COVID-19 and the multiple comorbidities associated with hematological malignancies.
血液系统恶性肿瘤患者因 COVID-19 导致的死亡率大幅上升。尽管 COVID-19 大流行的高峰期已经过去,但该病毒仍然常见,了解其对血液系统恶性肿瘤患者等弱势群体的影响仍然至关重要。关于大流行期间白血病和淋巴瘤患者的死亡率模式的研究有限。研究这些结果有助于深入了解 COVID-19 的不同浪潮如何影响免疫功能低下的个体,并支持制定预防、患者护理和降低风险的策略,这对于应对新出现的变种和预防未来的大流行至关重要。我们旨在确定美国白血病(LekCov-19)和淋巴瘤(LymCov-19)患者感染 COVID-19 的死亡风险以及 2020 年至 2021 年各四分位数之间的死亡率趋势。
我们分析了国家住院样本数据库(2020 - 2021 年),纳入因 COVID-19 入院的成年(≥18 岁)白血病和淋巴瘤患者。进行了描述性分析、倾向匹配和多变量回归,p 值≤0.05 被认为具有统计学意义。比较了各结果之间的死亡风险。
在 8191 例 LekCov-19 患者中,1200 例(14.7%)死亡,而 2578 例 LymCov-19 患者中有 507 例(19.7%)死亡。多变量回归显示 LekCOV-19 和 LymCOV-19 患者的死亡率增加了两倍(p < 0.001)。在两个队列中,包括肺、肾和心脏功能障碍在内的几种器官功能障碍与死亡率增加相关(p ≤ 0.0001)。同样,在两个队列中,骨髓功能障碍的迹象,如全血细胞减少和血小板减少,显示死亡几率增加(p < 0.01)。两个队列均呈现出不同的死亡率趋势,在 2020 年 10 月至 12 月、2021 年 1 月至 3 月、7 月至 9 月和 10 月至 12 月达到峰值(p ≤ 0.01)。造血干细胞移植受者在两个队列中的死亡几率较低,但未达到统计学意义(p > 0.05)。
COVID-19 与白血病和淋巴瘤患者的死亡率增加相关。已确定 2020 年 10 月至 2021 年 3 月期间 COVID-19 相关死亡率激增,这些趋势对于预测癌症患者未来的死亡风险可能至关重要。临床医生应优化治疗方案,并优先推进临床试验,以应对 COVID-19 的影响以及与血液系统恶性肿瘤相关的多种合并症。