Tupper Phoebe, Redfern Oliver, Harrison Charlotte H, Gerry Stephen, Biggs Christopher, Walker Bethany, Watkinson Peter
Critical Care Research Group, Kadoorie Centre for Critical Care Research and Education, Nuffield Department of Clinical Neurosciences, University of Oxford, Oxford, UK.
Centre for Statistics in Medicine, Nuffield Department of Orthopaedics, Rheumatology and Musculoskeletal Sciences, University of Oxford, Oxford, UK.
Age Ageing. 2025 Jul 1;54(7). doi: 10.1093/ageing/afaf194.
It has long been suspected that the vital sign abnormalities that accompany bacterial infection are subtle or absent in older adults. This review summarises the evidence for whether older adults present with different vital sign abnormalities to younger adults when hospitalised with bacterial infection.
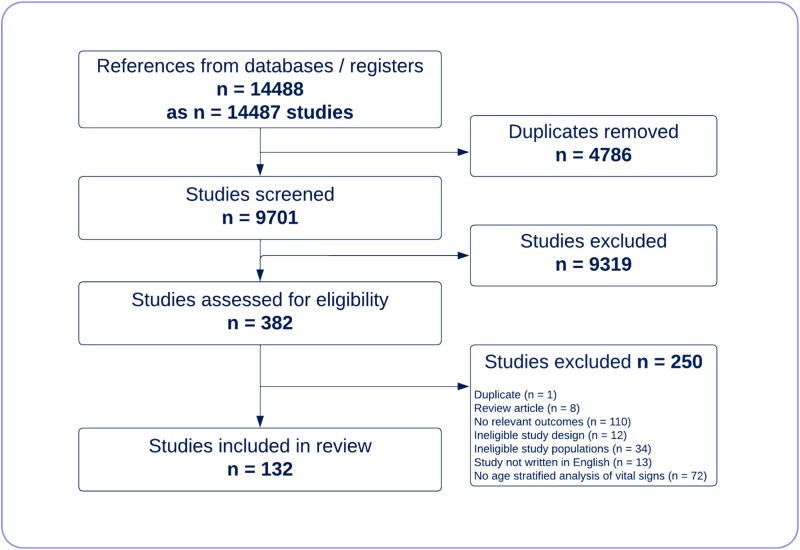
MEDLINE, EMBASE and CINAHL EBSCO were searched from inception to 19 December 2024 for English-language research articles of patients hospitalised with bacterial infection reporting age and admission vital signs. We used meta-regression to assess how vital signs vary with age. Where studies reported vital signs in multiple age groups, we undertook a meta-analysis in younger (<65) and older patients (≥65). Evidence quality was assessed using an adapted Quality Assessment of Diagnostic Accuracy Studies-2 tool.
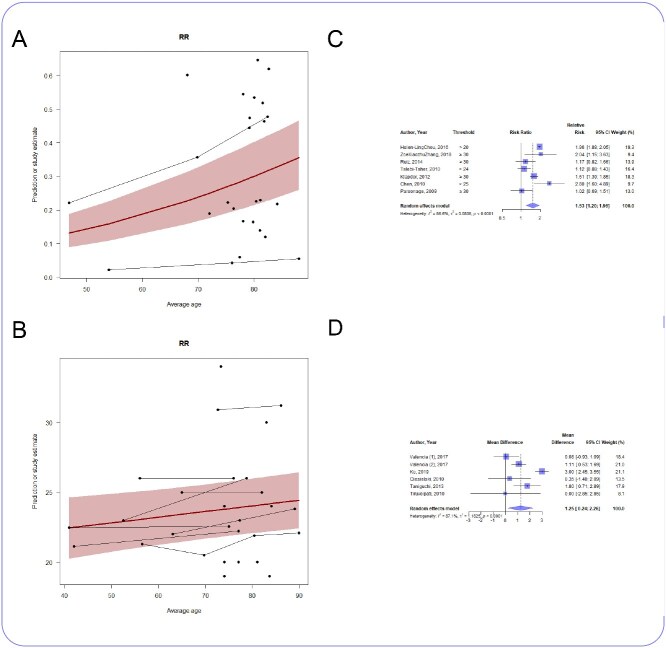
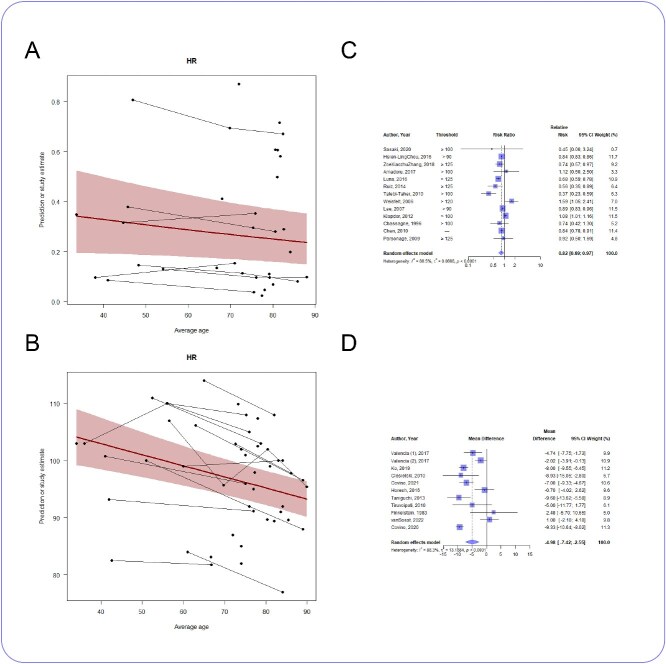
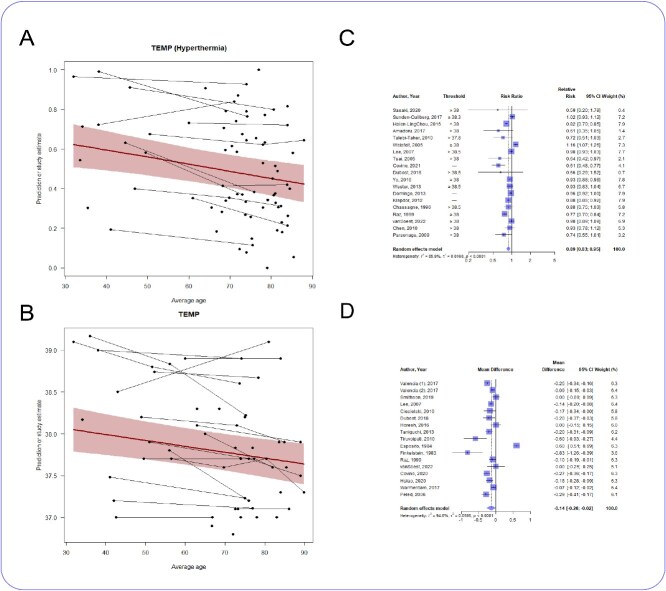
Our search yielded 14 487 studies; 132 were included after screening. Older adults were less likely to be tachycardic (RR 0.82, 0.69 to 0.97, I2 = 86.5%) with a mean difference in heart rate of 5 bpm (-7 to -3 bpm, I2 = 88.3%). Older adults were less likely to be febrile (RR 0.89, 0.83 to 0.95, I2 = 85.9%) with a mean difference in temperature of 0.14°C (-0.26 to -0.02°C, I2 = 94.6%). Most (129/132) studies were at high risk of bias.
Whilst differences in absolute values were small, there was consistency in the finding that older adults were less likely than younger adults to be tachycardic or febrile. As vital signs at presentation may prompt suspicion of infection, influencing investigations and treatment, special consideration for the possibility of infection in older patients with normal vital signs may be warranted.
长期以来,人们一直怀疑老年人在细菌感染时生命体征异常不明显或不存在。本综述总结了关于老年人与年轻人在因细菌感染住院时生命体征异常是否存在差异的证据。
检索MEDLINE、EMBASE和CINAHL EBSCO数据库,从建库至2024年12月19日,查找报道了年龄和入院时生命体征的因细菌感染住院患者的英文研究文章。我们使用meta回归分析评估生命体征如何随年龄变化。若研究报告了多个年龄组的生命体征,我们对年轻患者(<65岁)和老年患者(≥65岁)进行了meta分析。使用改编后的诊断准确性研究质量评估-2工具评估证据质量。
我们的检索共得到14487项研究;筛选后纳入132项。老年人出现心动过速的可能性较小(风险比0.八二,0.69至0.97,I² = 86.5%),心率平均差异为5次/分钟(-7至-3次/分钟,I² = 88.3%)。老年人发热的可能性较小(风险比0.89,0.83至0.95,I² = 85.9%),体温平均差异为0.14°C(-0.26至-0.02°C,I² = 94.6%)。大多数(129/132)研究存在高偏倚风险。
虽然绝对值差异较小,但老年人比年轻人更不容易出现心动过速或发热这一发现具有一致性。由于就诊时的生命体征可能会引发对感染的怀疑,影响检查和治疗,因此对于生命体征正常的老年患者感染可能性应给予特别考虑。