Xie Jun, Zhu Yang, Wang Ya, Mo Yunjun, Shi Xiaohui, Liang Wen-Ming, Ren Fei-Fei, Bai Zhenmin, Nie Feng
Department of Rehabilitation Medicine, Chengdu Seventh People's Hospital, Affiliated Cancer Hospital of Chengdu Medical College, Chengdu, China.
School of Sports Medicine and Rehabilitation, Beijing Sport University, Beijing, China.
Front Med (Lausanne). 2025 Jul 9;12:1621375. doi: 10.3389/fmed.2025.1621375. eCollection 2025.
Pulmonary rehabilitation is central to COPD management, with inspiratory muscle training (IMT) as a key component. However, evidence is inconsistent on whether combining PR with IMT offers added benefits for older COPD patients.
To evaluate the comparative effects of PR combined with IMT versus PR alone on key outcomes in older COPD patients, including quality of life [St. George's Respiratory Questionnaire (SGRQ)], exercise tolerance [6-min walk distance (6MWD)], respiratory muscle strength [maximal inspiratory pressure (PImax)], and pulmonary function metrics (FEV, FEV%).
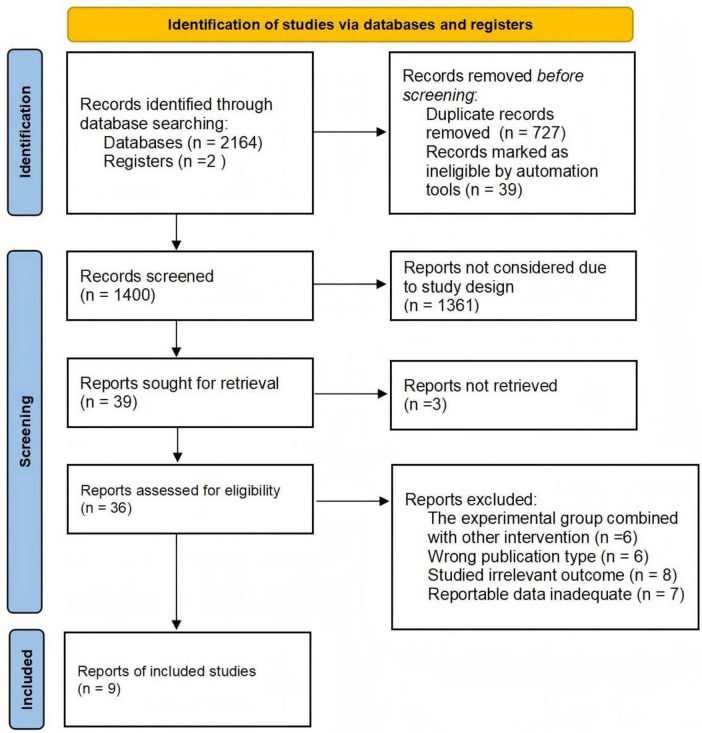
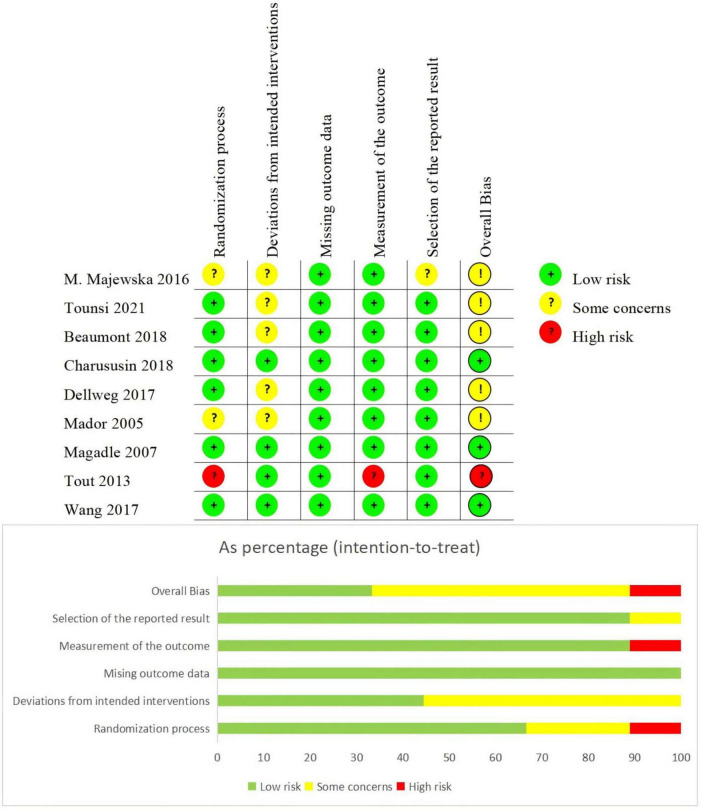
A systematic search of PubMed, EMBASE, Web of Science, and the Cochrane Library (January 2005-January 2025) identified randomized controlled trials (RCTs) meeting criteria: (1) participants were ≥ 55 years old with GOLD stage II-IV COPD; (2) interventions compared PR combined with IMT versus PR alone; (3) outcomes included PImax, FEV, FEV%, SGRQ, and 6MWD. Non-English and animal studies were excluded. Risk of bias was assessed using Cochrane RoB 2.0, and the certainty of evidence was evaluated via the GRADEpro 3.6.1.
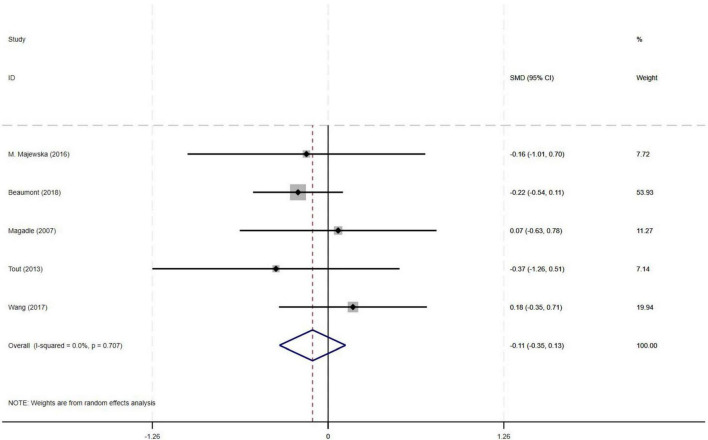
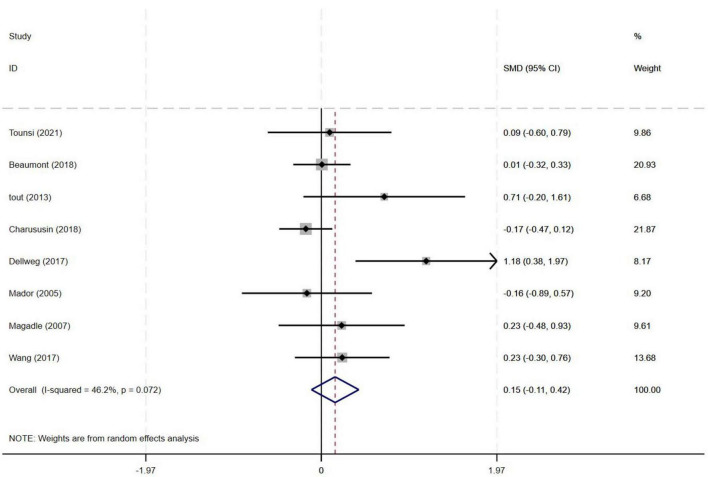
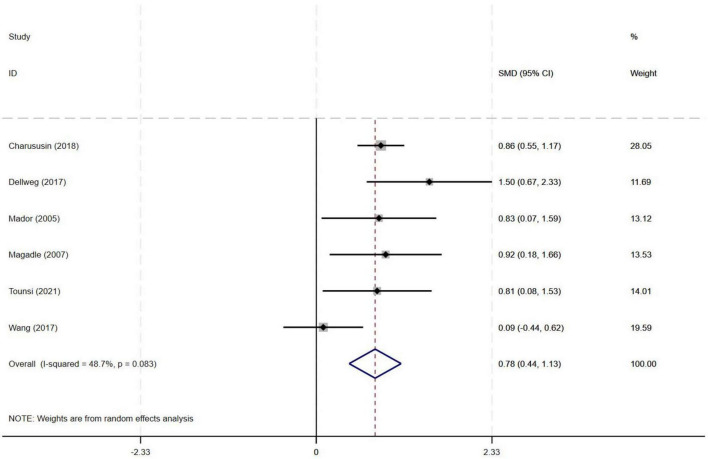
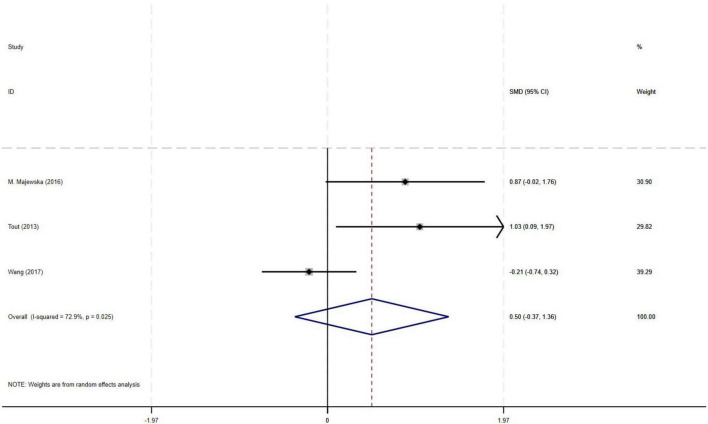
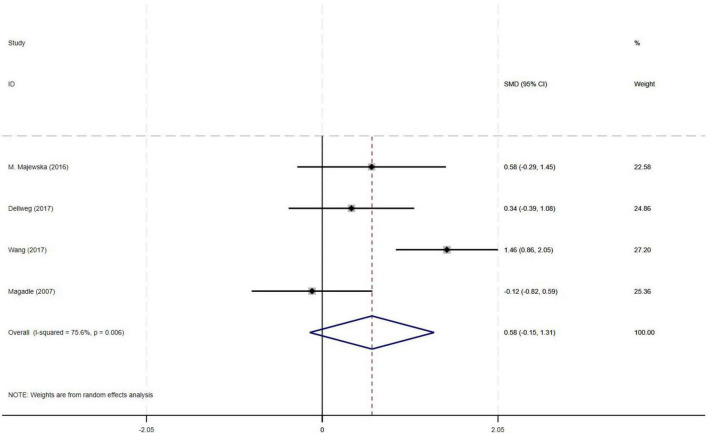
Nine RCTs (582 patients) were included. Compared with PR alone, PR combined with IMT did not improve 6MWD (SMD = 0.15, 95% CI: -0.11-0.42; low-quality evidence) or SGRQ scores (SMD = -0.19, 95% CI: -0.38-0.01, low-quality evidence). PImax improved moderately (SMD = 0.78, 95% CI: 0.44-1.13, I = 48.7%, low-quality evidence). FEV and FEV% trended upward (SMD = 0.50 and 0.58, respectively) but showed high heterogeneity (FEV: I = 72.9%, = 0.025, very low-quality evidence; FEV%: I = 75.6%, = 0.006, low-quality evidence), precluding significance. Subgroup analyses showed significant PImax improvements in interventions lasting ≥ 12 weeks (SMD = 0.866, 95% CI: 0.579-1.153; I = 0%) or with weekly cumulative durations ≥ 180 min (SMD = 0.922, 95% CI: 0.666-1.177; I = 0%), with no 6MWD benefits in any subgroup.
Low-quality evidence indicates that PR combined with IMT improves respiratory muscle strength (PImax) in older COPD patients versus PR alone, with no significant benefit for exercise capacity (6MWD) or lung function. For older COPD patients, ≥ 12-week PR combined with IMT interventions (sessions > 60 min; weekly duration ≥ 180 min) may enhance PImax.
https://www.crd.york.ac.uk/PROSPERO/view/CRD420251010168, CRD420251010168.
肺康复是慢性阻塞性肺疾病(COPD)管理的核心内容,吸气肌训练(IMT)是其中的关键组成部分。然而,对于老年COPD患者,肺康复联合吸气肌训练是否能带来额外益处,相关证据并不一致。
评估肺康复联合吸气肌训练与单纯肺康复相比,对老年COPD患者关键结局指标的影响,这些指标包括生活质量[圣乔治呼吸问卷(SGRQ)]、运动耐力[6分钟步行距离(6MWD)]、呼吸肌力量[最大吸气压(PImax)]以及肺功能指标(第1秒用力呼气容积(FEV₁)、FEV₁占预计值百分比)。
系统检索PubMed、EMBASE、科学引文索引(Web of Science)和考克兰图书馆(2005年1月至2025年1月),以确定符合以下标准的随机对照试验(RCT):(1)参与者年龄≥55岁,GOLD分级为II-IV级COPD;(2)干预措施比较了肺康复联合吸气肌训练与单纯肺康复;(3)结局指标包括PImax、FEV₁、FEV₁占预计值百分比、SGRQ和6MWD。排除非英文研究和动物研究。使用考克兰偏倚风险评估工具2.0评估偏倚风险,并通过GRADEpro 3.6.1评估证据的确定性。
纳入9项RCT(582例患者)。与单纯肺康复相比,肺康复联合吸气肌训练并未改善6分钟步行距离(标准化均数差(SMD)=0.15,95%置信区间(CI):-0.11-0.42;低质量证据)或SGRQ评分(SMD=-0.19,95%CI:-0.38-0.01,低质量证据)。最大吸气压有中度改善(SMD=0.78,95%CI:0.44-1.13,I²=48.7%,低质量证据)。第1秒用力呼气容积和FEV₁占预计值百分比呈上升趋势(SMD分别为0.50和0.58),但异质性较高(第1秒用力呼气容积:I²=72.9%,P=0.025,极低质量证据;FEV₁占预计值百分比:I²=75.6%,P=0.006,低质量证据),无法得出显著结论。亚组分析显示,持续时间≥12周的干预措施(SMD=0.866,95%CI:0.579-1.153;I²=0%)或每周累计时长≥180分钟的干预措施(SMD=0.922,95%CI:0.666-1.177;I²=0%)中,最大吸气压有显著改善,各亚组在6分钟步行距离方面均未获益。
低质量证据表明,与单纯肺康复相比,肺康复联合吸气肌训练可改善老年COPD患者的呼吸肌力量(最大吸气压),但对运动能力(6分钟步行距离)或肺功能无显著益处。对于老年COPD患者,≥12周的肺康复联合吸气肌训练干预(每次时长>60分钟;每周时长≥180分钟)可能会增强最大吸气压。
https://www.crd.york.ac.uk/PROSPERO/view/CRD420251010168,CRD420251010168 。