Benghanem Sarah, Novy Jan, Schindler Kaspar A, Rüegg Stephan, Alvarez Vincent, Rossetti A O
Department of Clinical Neurosciences, Lausanne University Hospital (CHUV), University of Lausanne, Lausanne, Switzerland.
Medical ICU, Cochin Hospital, APHP Centre, Paris, France.
Eur J Neurol. 2025 Aug;32(8):e70312. doi: 10.1111/ene.70312.
Prognostication of neurological outcome in critically ill patients presents significant challenges. While EEG reactivity may be associated with outcome in hypoxic-ischemic brain injury (HIBI), it has received scarce attention in other etiological conditions. Our objective was to investigate the association of EEG reactivity to clinical outcome in patients with disorders of consciousness of various etiologies.
This is an ancillary study of the randomized CERTA trial (NCT03129438), which included adults with disorders of consciousness randomized to continuous EEG for 30-48 h or two routine EEGs (20-30 min). We explored the association between EEG characteristics and neurological outcome at 6 months, a modified Rankin Scale (mRS) 3-6 being considered unfavorable.
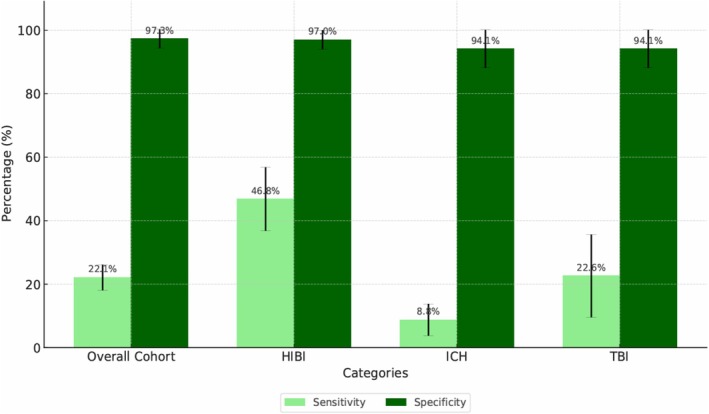
A total of 364 patients were included. Among them, 112 patients had HIBI, 85 intracranial hemorrhage (ICH), 28 ischemic stroke, 48 traumatic brain injury (TBI), 23 toxic-metabolic encephalopathy, 7 encephalitis, and 114 had unknown or other etiologies. In the overall cohort, abnormal background continuity (OR 2.33, 95% CI [1.15-4.76], p = 0.019), ictal-interictal continuum features (OR 2.78, 95% CI [1.16-6.67], p = 0.021) and unreactive background (OR 10.9, 95% CI [1.97-58.82], p = 0.006) were independently associated with unfavorable outcome. In the overall cohort, unreactive EEG had specificity of 97.3% (95% CI [94.3-100]) and sensitivity of 22.1% (95% CI [17-27.2]) for unfavorable outcome. In HIBI, specificity was 97% (95% CI [91.1-100]) and sensitivity 46.8% (95% CI [35.8-57.8]); in ICH, specificity was 94.1% (95% CI [83-100]) and sensitivity 8.8% (95% CI [2.05-15.55]); in TBI, specificity was 94.1% (95% CI [83-100]) and sensitivity 22.6% (95% CI [7.8-37.3]).
In this etiologically mixed cohort of critically ill adults, unreactive EEG predicted unfavorable outcome at 6 months with high specificity. EEG reactivity may reduce prognostic uncertainty not only for patients with HIBI, but also for other types of acute brain injury, such as TBI and ICH.
对重症患者的神经功能预后进行预测面临重大挑战。虽然脑电图反应性可能与缺氧缺血性脑损伤(HIBI)的预后相关,但在其他病因情况下,它很少受到关注。我们的目的是研究各种病因导致的意识障碍患者脑电图反应性与临床预后之间的关联。
这是一项对随机CERTA试验(NCT03129438)的辅助研究,该试验纳入了意识障碍的成年人,随机分为接受30 - 48小时连续脑电图监测或两次常规脑电图监测(20 - 30分钟)。我们探讨了脑电图特征与6个月时神经功能预后之间的关联,改良Rankin量表(mRS)评分为3 - 6分被视为不良预后。
共纳入364例患者。其中,112例为HIBI,85例为颅内出血(ICH),28例为缺血性中风,48例为创伤性脑损伤(TBI),23例为中毒代谢性脑病,7例为脑炎,114例病因不明或为其他病因。在整个队列中,背景连续性异常(比值比2.33,95%可信区间[1.15 - 4.76],p = 0.019)、发作期 - 发作间期连续特征(比值比2.78,95%可信区间[1.16 - 6.67],p = 0.021)和无反应性背景(比值比10.9,95%可信区间[1.97 - 58.82],p = 0.006)与不良预后独立相关。在整个队列中,无反应性脑电图对不良预后的特异性为97.3%(95%可信区间[94.3 - 100]),敏感性为22.1%(95%可信区间[17 - 27.2])。在HIBI中,特异性为97%(95%可信区间[91.1 - 100]),敏感性为46.8%(95%可信区间[35.8 - 57.8]);在ICH中,特异性为94.1%(95%可信区间[83 - 100]),敏感性为8.8%(95%可信区间[2.05 - 15.55]);在TBI中,特异性为94.1%(95%可信区间[83 - 100]),敏感性为22.6%(95%可信区间[7.8 - 37.3])。
在这个病因混杂的重症成年患者队列中,无反应性脑电图以高特异性预测6个月时的不良预后。脑电图反应性不仅可能降低HIBI患者的预后不确定性,也可能降低其他类型急性脑损伤(如TBI和ICH)患者的预后不确定性。