Sorbonne Université, Paris, France.
Paris Brain Institute - ICM, Inserm, CNRS, PICNIC-Lab, Paris, France.
Nat Med. 2024 Aug;30(8):2349-2355. doi: 10.1038/s41591-024-03019-1. Epub 2024 May 30.
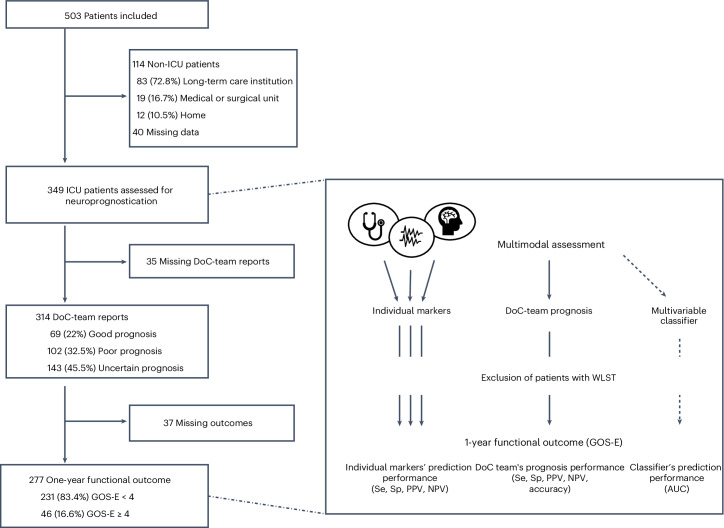
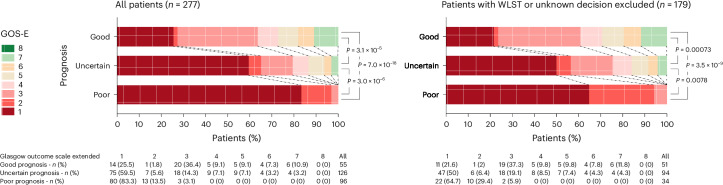
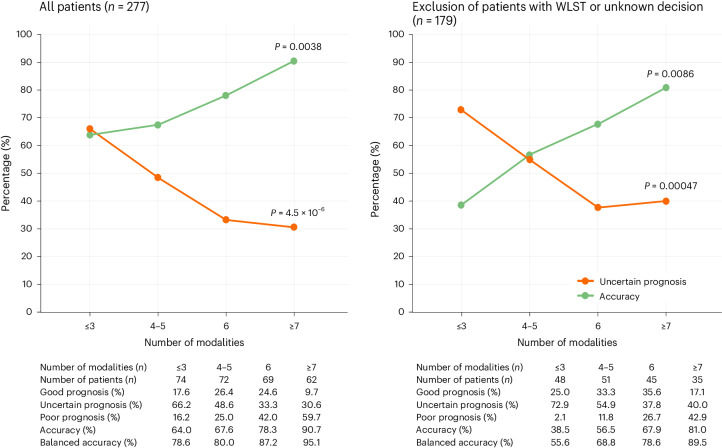
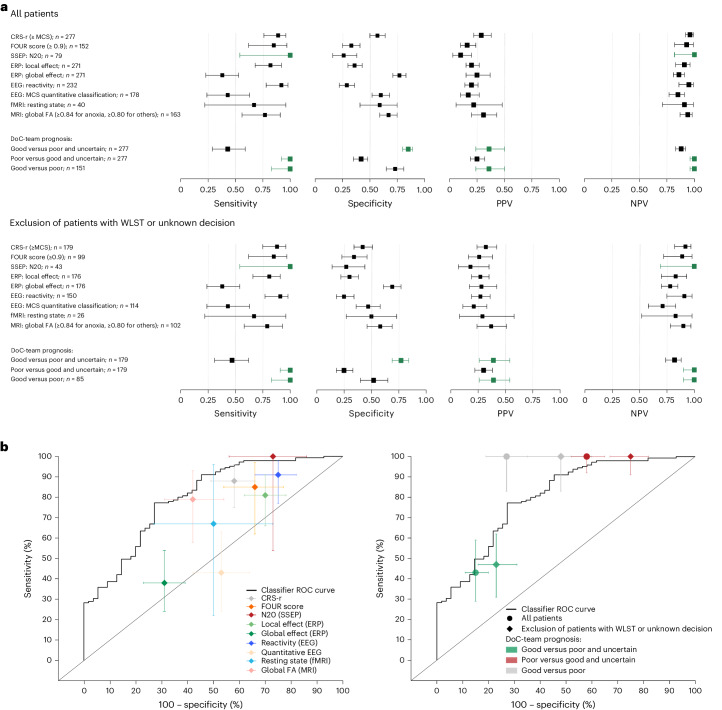
Accurately predicting functional outcomes for unresponsive patients with acute brain injury is a medical, scientific and ethical challenge. This prospective study assesses how a multimodal approach combining various numbers of behavioral, neuroimaging and electrophysiological markers affects the performance of outcome predictions. We analyzed data from 349 patients admitted to a tertiary neurointensive care unit between 2009 and 2021, categorizing prognoses as good, uncertain or poor, and compared these predictions with observed outcomes using the Glasgow Outcome Scale-Extended (GOS-E, levels ranging from 1 to 8, with higher levels indicating better outcomes). After excluding cases with life-sustaining therapy withdrawal to mitigate the self-fulfilling prophecy bias, our findings reveal that a good prognosis, compared with a poor or uncertain one, is associated with better one-year functional outcomes (common odds ratio (95% CI) for higher GOS-E: OR = 14.57 (5.70-40.32), P < 0.001; and 2.9 (1.56-5.45), P < 0.001, respectively). Moreover, increasing the number of assessment modalities decreased uncertainty (OR = 0.35 (0.21-0.59), P < 0.001) and improved prognostic accuracy (OR = 2.72 (1.18-6.47), P = 0.011). Our results underscore the value of multimodal assessment in refining neuroprognostic precision, thereby offering a robust foundation for clinical decision-making processes for acutely brain-injured patients. ClinicalTrials.gov registration: NCT04534777 .
准确预测急性脑损伤无反应患者的功能预后是一个医学、科学和伦理方面的挑战。本前瞻性研究评估了结合多种行为、神经影像学和电生理学标志物的多模态方法如何影响预后预测的性能。我们分析了 2009 年至 2021 年间入住三级神经重症监护病房的 349 名患者的数据,将预后分为良好、不确定或不良,并使用格拉斯哥预后量表扩展版(GOS-E,范围从 1 到 8,分数越高表示预后越好)比较这些预测与观察到的结果。在排除因维持生命治疗而退出的病例以减轻自我实现预言偏见后,我们的研究结果表明,与预后不良或不确定相比,预后良好与一年后更好的功能结局相关(更高 GOS-E 的常见优势比(95%置信区间):OR=14.57(5.70-40.32),P<0.001;和 2.9(1.56-5.45),P<0.001)。此外,增加评估方式的数量可以降低不确定性(OR=0.35(0.21-0.59),P<0.001)并提高预后准确性(OR=2.72(1.18-6.47),P=0.011)。我们的研究结果强调了多模态评估在提高神经预后精度方面的价值,从而为急性脑损伤患者的临床决策过程提供了可靠的基础。ClinicalTrials.gov 注册号:NCT04534777。