Kleinová Patrícia, Vnučák Matej, Graňák Karol, Beliančinová Monika, Blichová Tímea, Dedinská Ivana
Transplant-Nephrology Department, University Hospital Martin, Kollárova 2, 03601 Martin, Slovakia.
Department of Internal Medicine I, Jessenius Medical Faculty, Comenius University, 03601 Martin, Slovakia.
Reports (MDPI). 2024 Aug 13;7(3):70. doi: 10.3390/reports7030070.
Prostate cancer is the most common malignancy in men. Secondary nephrotic syndrome, a feature of paraneoplastic syndrome, occurs in 11% of cases and is mainly caused by membranous glomerulopathy. The association between minimal change disease and prostate cancer is rare. Only one cause has been described in the available literature.
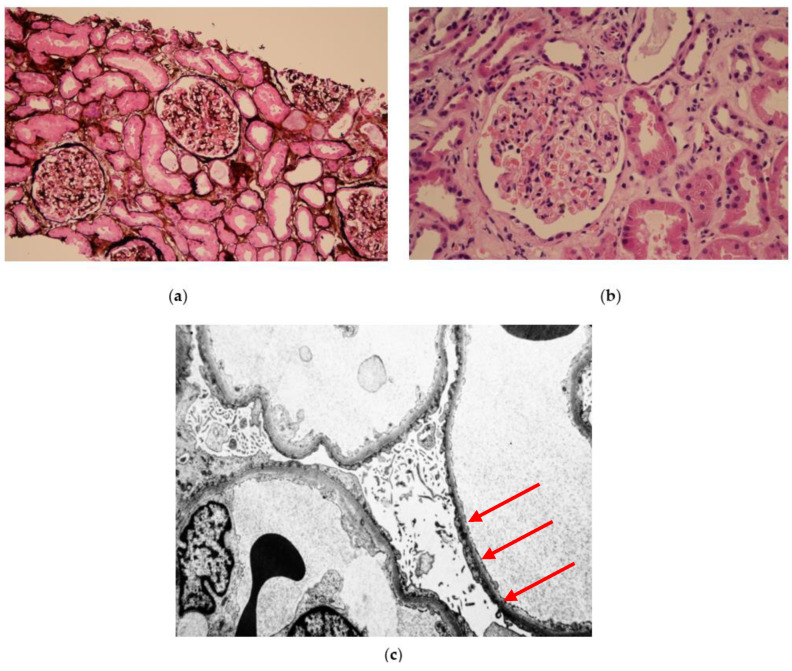
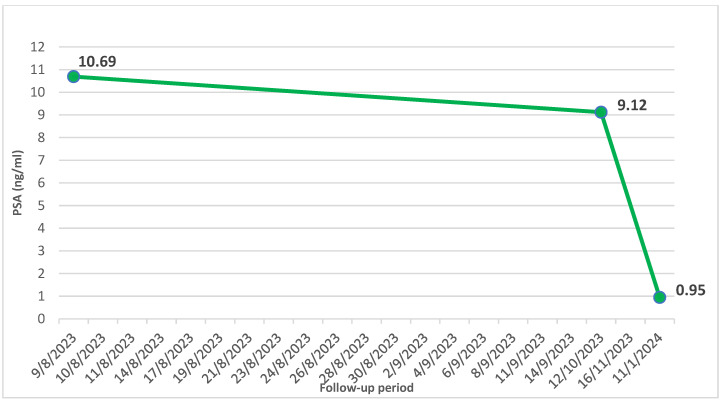
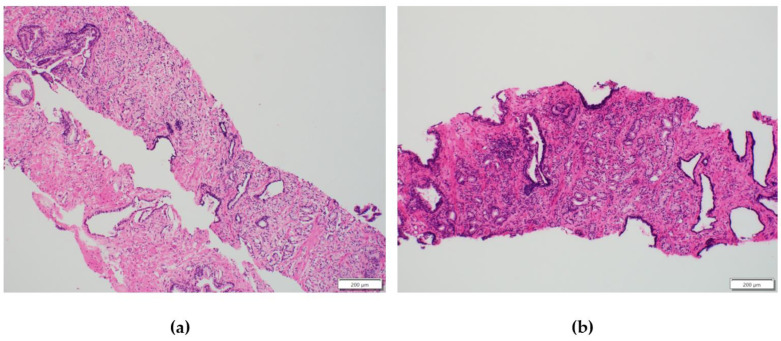
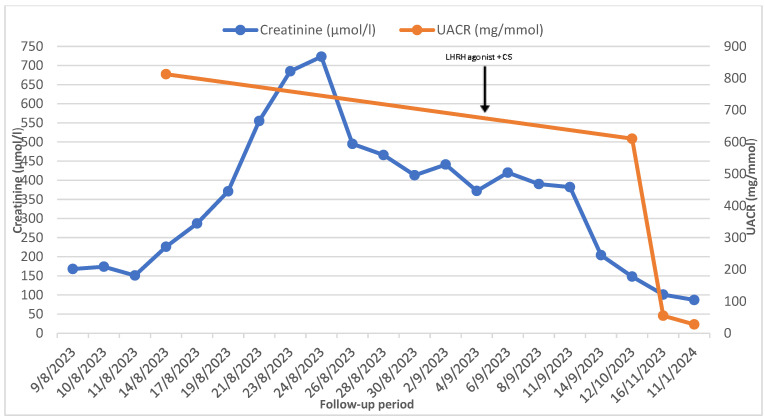
We present the case of a 77-year-old patient who was admitted to our department with stage 3 acute kidney injury and with nephrotic syndrome with anasarca (creatinine: 168 µmol/L, eGFR: 33 mL/min/1.73 m, albumin: 18.5 g/L, total cholesterol: 6.86 mmol/L, urine albumin creatinine ratio: 812.7 mg/mmol). In the differential diagnosis of nephrotic syndrome, looking for a secondary cause is essential, so the parainfectious causes of nephrotic syndrome were excluded. An elevated prostate-specific antigen (10.69 ng/L) was found when screening for oncological causes, and prostate adenocarcinoma was identified on biopsy. A renal biopsy was then performed with a finding of minimal change disease. Despite the generally accepted guidelines of prostate carcinoma in that stage and age of the patient being watchful waiting, antiandrogen therapy was started with the cooperation of a urologist. There was a significant improvement in renal parameters in the patient (creatinine: 87 µmol/L, eGFR: 73 mL/min/1.73 m, albumin: 33.4 g/L, urine albumin creatinine ratio: 27.6 mg/mmol).
This case shows the importance of multidisciplinary cooperation in the treatment of secondary causes of nephrotic syndrome. In the case of proven paraneoplastic syndrome, it is necessary to start treating the malignancy; however, in general, a conservative approach without treatment is recommended.
前列腺癌是男性最常见的恶性肿瘤。继发性肾病综合征是副肿瘤综合征的一个特征,在11%的病例中出现,主要由膜性肾小球病引起。微小病变病与前列腺癌之间的关联很少见。现有文献中仅描述了一例病因。
我们报告了一例77岁患者,因3期急性肾损伤和伴有全身性水肿的肾病综合征入住我科(肌酐:168 μmol/L,估算肾小球滤过率:33 mL/min/1.73 m²,白蛋白:18.5 g/L,总胆固醇:6.86 mmol/L,尿白蛋白肌酐比值:812.7 mg/mmol)。在肾病综合征的鉴别诊断中,寻找继发性病因至关重要,因此排除了肾病综合征的感染后病因。在筛查肿瘤病因时发现前列腺特异性抗原升高(10.69 ng/L),活检确诊为前列腺腺癌。随后进行肾活检,结果为微小病变病。尽管对于该患者所处阶段和年龄的前列腺癌,普遍接受的指南是密切观察等待,但在泌尿科医生的合作下开始了抗雄激素治疗。患者的肾脏参数有显著改善(肌酐:87 μmol/L,估算肾小球滤过率:73 mL/min/1.73 m²,白蛋白:33.4 g/L,尿白蛋白肌酐比值:27.6 mg/mmol)。
本病例显示了多学科合作在治疗肾病综合征继发性病因中的重要性。在确诊为副肿瘤综合征的情况下,有必要开始治疗恶性肿瘤;然而,一般而言,建议采取不进行治疗的保守方法。