Yoo Seung Hee, Beak Min Hyouk, Lee Dong Hyeon, Kim Won-Joong
Department of Anesthesiology and Pain Medicine, College of Medicine, Ewha Womans University, Ewha Womans University Mokdong Hospital, Seoul 07985, Republic of Korea.
Department of Urology, College of Medicine, Ewha Womans University, Ewha Womans University Mokdong Hospital, Seoul 07985, Republic of Korea.
J Clin Med. 2025 Jul 22;14(15):5186. doi: 10.3390/jcm14155186.
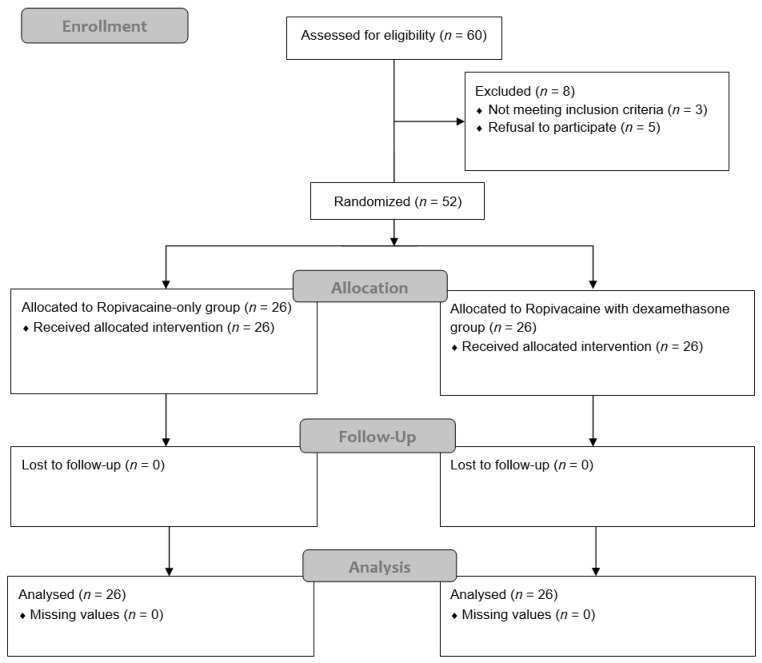
: Radical cystectomy performed via midline laparotomy is associated with substantial postoperative pain, frequently necessitating a high opioid consumption, which may impair immune function and delay recovery. The rectus sheath block (RSB) is widely used as part of multimodal analgesia to enhance postoperative pain control; however, the duration of analgesia is limited when using single-injection techniques. Dexamethasone has increasingly been used as a perineural adjuvant to prolong the effects of peripheral nerve blocks and enhance analgesia. This randomized controlled trial evaluated whether adding perineural dexamethasone to an RSB improves analgesic efficacy in patients undergoing a radical cystectomy. : Fifty-two adult patients scheduled for radical cystectomy were randomly assigned to receive an ultrasound-guided bilateral RSB with either 0.25% ropivacaine alone or 0.25% ropivacaine combined with 4 mg dexamethasone per side after skin closure. Postoperative pain was assessed using a numeric rating scale (NRS) at 3, 6, 12, 18, 24, and 48 h following surgery. Cumulative intravenous patient-controlled analgesia (IV-PCA) in terms of fentanyl consumption and the incidence of rebound pain-defined as an increase in the NRS from ≤3 to ≥7 within 24 h after the block administration-were also recorded. : The dexamethasone group exhibited significantly reduced cumulative fentanyl consumption. Pain scores were consistently lower in the dexamethasone group compared with the ropivacaine-only group at all time points except 3 h postoperatively. The incidence of rebound pain was also substantially lower in the dexamethasone group. : Perineural dexamethasone as an adjuvant to an RSB provides effective and prolonged analgesia, reduces opioid requirements, and lowers rebound pain incidence in patients undergoing a radical cystectomy.
经中线剖腹术进行根治性膀胱切除术会导致严重的术后疼痛,常常需要大量使用阿片类药物,这可能会损害免疫功能并延迟恢复。腹直肌鞘阻滞(RSB)作为多模式镇痛的一部分被广泛应用,以加强术后疼痛控制;然而,使用单次注射技术时镇痛持续时间有限。地塞米松越来越多地被用作神经周围佐剂,以延长周围神经阻滞的效果并增强镇痛作用。这项随机对照试验评估了在接受根治性膀胱切除术的患者中,在RSB中添加神经周围地塞米松是否能提高镇痛效果。:52例计划进行根治性膀胱切除术的成年患者被随机分配,在皮肤缝合后接受超声引导下双侧RSB,一侧单独使用0.25%罗哌卡因,或一侧使用0.25%罗哌卡因并联合4mg地塞米松。术后3、6、12、18、24和48小时使用数字评分量表(NRS)评估术后疼痛。还记录了芬太尼消耗量方面的累积静脉自控镇痛(IV-PCA)以及反弹痛的发生率(定义为在阻滞给药后24小时内NRS从≤3增加到≥7)。:地塞米松组的累积芬太尼消耗量显著降低。除术后3小时外,地塞米松组在所有时间点的疼痛评分均始终低于仅使用罗哌卡因组。地塞米松组的反弹痛发生率也显著更低。:神经周围地塞米松作为RSB的佐剂,可为接受根治性膀胱切除术的患者提供有效且持久的镇痛,减少阿片类药物需求,并降低反弹痛发生率。