Stanciu Ionut-Valentin, Fildan Ariadna-Petronela, Ilie Adrian Cosmin, Oancea Cristian, Stanga Livia, Tudorache Emanuela, Bratosin Felix, Rosca Ovidiu, Bogdan Iulia, Tofolean Doina-Ecaterina, Preotesoiu Ionela, Zamfir Viorica, Dantes Elena
Faculty of Medicine, "Ovidius" University of Constanta, 900470 Constanta, Romania.
Doctoral School of Medicine, "Ovidius" University of Constanta, 900470 Constanta, Romania.
J Clin Med. 2025 Jul 28;14(15):5327. doi: 10.3390/jcm14155327.
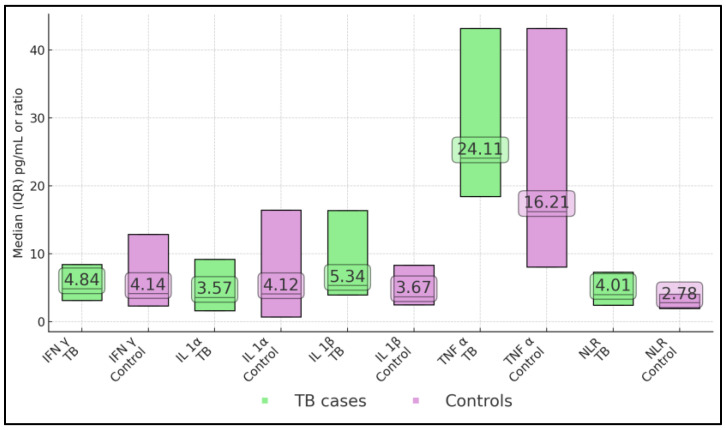
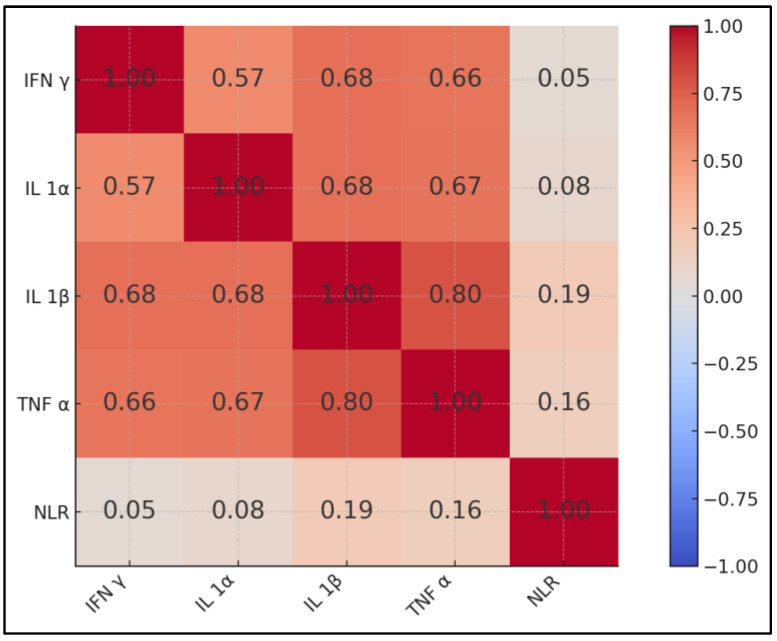
Romania remains a tuberculosis (TB) hotspot in the European Union, yet host-derived factors of poor outcomes are poorly characterised. We quantified circulating pro-inflammatory cytokines and examined their interplay with behavioural risk factors, the nutritional status, and the clinical course in adults hospitalised with pulmonary TB. We analysed 80 adults with microbiologically confirmed pulmonary TB and 40 respiratory symptom controls; four TB patients (5%) died during hospitalisation, all within 10 days of admission. A retrospective analytical case-control study was conducted at the Constanța regional TB referral centre (October 2020-October 2023). Patients with smear- or culture-confirmed TB were frequency-matched by sex, 10-year age band, and BMI class to culture-negative respiratory controls at a 2:1 ratio. The patients' serum interferon-γ (IFN-γ), interleukin-1α (IL-1α), interleukin-1β (IL-1β), and tumour-necrosis-factor-α (TNF-α) were quantified within 24 h of admission; the neutrophil/lymphocyte ratio (NLR) was extracted from full blood counts. Independent predictors of in-hospital mortality were identified by multivariable logistic regression; factors associated with the length of stay (LOS) were modelled with quasi-Poisson regression. The median TNF-α (24.1 pg mL vs. 16.2 pg mL; = 0.009) and IL-1β (5.34 pg mL vs. 3.67 pg mL; = 0.008) were significantly higher in the TB cases than in controls. TNF-α was strongly correlated with IL-1β (ρ = 0.80; < 0.001), while NLR showed weak concordance with multiplex cytokine patterns. Among the patients with TB, four early deaths (5%) exhibited a tripling of TNF-α (71.4 pg mL) and a doubling of NLR (7.8) compared with the survivors. Each 10 pg mL rise in TNF-α independently increased the odds of in-hospital death by 1.8-fold (95% CI 1.1-3.0; = 0.02). The LOS (median 29 days) was unrelated to the smoking, alcohol, or comorbidity load, but varied across BMI strata: underweight, 27 days; normal weight, 30 days; overweight, 23 days (Kruskal-Wallis = 0.03). In a multivariable analysis, under-nutrition (BMI < 18.5 kg m) prolonged the LOS by 19% (IRR 1.19; 95% CI 1.05-1.34; = 0.004) independently of the disease severity. A hyper-TNF-α/IL-1β systemic signature correlates with early mortality in Romanian pulmonary TB, while under-nutrition is the dominant modifiable determinant of prolonged hospitalisation. Admission algorithms that pair rapid TNF-α testing with systematic nutritional assessment could enable targeted host-directed therapy trials and optimise bed utilisation in high-burden settings.
罗马尼亚仍是欧盟的结核病热点地区,但宿主因素导致的不良预后特征尚不明确。我们对循环促炎细胞因子进行了定量分析,并研究了它们与行为风险因素、营养状况以及成年肺结核住院患者临床病程之间的相互作用。我们分析了80例微生物学确诊的成年肺结核患者和40例有呼吸道症状的对照者;4例肺结核患者(5%)在住院期间死亡,均在入院后10天内。在康斯坦察地区结核病转诊中心(2020年10月至2023年10月)进行了一项回顾性分析病例对照研究。涂片或培养确诊的结核病患者按性别、10岁年龄组和BMI类别与培养阴性的呼吸道对照者以2:1的比例进行频率匹配。在入院后24小时内对患者血清中的干扰素-γ(IFN-γ)、白细胞介素-1α(IL-1α)、白细胞介素-1β(IL-β)和肿瘤坏死因子-α(TNF-α)进行定量;从全血细胞计数中提取中性粒细胞/淋巴细胞比值(NLR)。通过多变量逻辑回归确定住院死亡率的独立预测因素;用准泊松回归对与住院时间(LOS)相关的因素进行建模。结核病病例组的TNF-α中位数(24.1 pg/mL对16.2 pg/mL;P = 0.009)和IL-1β中位数(5.34 pg/mL对3.67 pg/mL;P = 0.008)显著高于对照组。TNF-α与IL-1β高度相关(ρ = 0.80;P < 0.001),而NLR与多种细胞因子模式的一致性较弱。在结核病患者中,4例早期死亡(5%)的TNF-α增加了两倍(71.4 pg/mL),NLR增加了一倍(7.8),而幸存者则不然。TNF-α每升高10 pg/mL,住院死亡几率独立增加1.8倍(95%CI 1.1 - 3.0;P = 0.02)。住院时间(中位数29天)与吸烟、饮酒或合并症负担无关,但在不同BMI分层中有所不同:体重过轻患者为27天;正常体重患者为30天;超重患者为23天(Kruskal-Wallis检验,P = 0.03)。在多变量分析中,营养不良(BMI < 18.5 kg/m²)使住院时间延长19%(IRR 1.19;95%CI 1.05 - 1.34;P = 0.004),且与疾病严重程度无关。高TNF-α/IL-1β全身特征与罗马尼亚肺结核患者的早期死亡率相关,而营养不良是住院时间延长的主要可改变决定因素。将快速TNF-α检测与系统营养评估相结合的入院算法,可促成有针对性的宿主导向治疗试验,并在高负担环境中优化床位利用。