Benedetti E, Troppmann C, Gillingham K, Sutherland D E, Payne W D, Dunn D L, Matas A J, Najarian J S, Grussner R W
Department of Surgery, University of Minnesota, Minneapolis, USA.
Ann Surg. 1995 Apr;221(4):406-14. doi: 10.1097/00000658-199504000-00012.
The authors determined whether the use of kidney allografts with multiple renal arteries adversely effects post-transplant graft and patient outcome or increases the incidence of vascular and urologic complications.
Kidney grafts with multiple renal arteries have been associated with an increased incidence of early vascular and urologic complications. Kidney transplants with single versus multiple renal arteries have not been compared in regard to long-term graft and patient outcome or post-transplant incidence of hypertension, acute tubular necrosis, rejection, and late vascular and urologic complications.
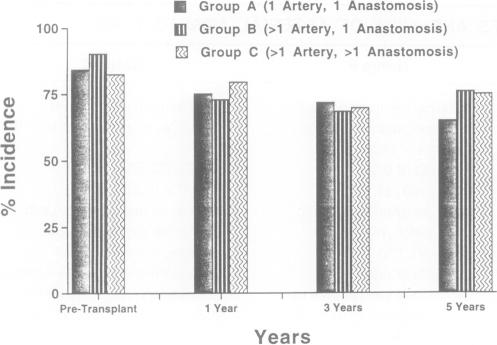
We analyzed 998 adult kidney transplants done from December 1, 1985 through June 30, 1993, in which only the recipient's external or internal iliac artery was used for anastomosis. We divided the study population into 3 groups: Group A-1 renal artery, 1 arterial anastomosis (n = 835), Group B-->1 renal artery, 1 arterial anastomosis (n = 112), Group C-->1 renal artery, > 1 arterial anastomosis (n = 51). We compared the incidence of post-transplant hypertension, acute tubular necrosis, acute rejection, and vascular and urologic complications; mean creatinine levels at 1, 3, and 5 years post-transplant; and patient and graft survival. Univariate and multivariate analyses were done to identify risk factors for vascular complications.
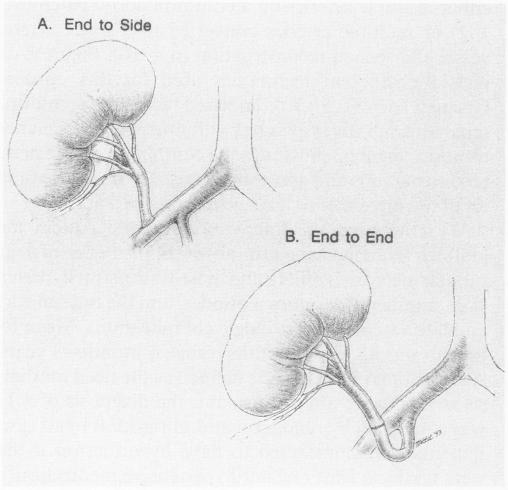
We found no significant differences among the three groups for the following variables: post-transplant hypertension, acute tubular necrosis, acute rejection, creatinine levels, early vascular and urologic complications, and graft and patient survival. In kidneys with single arteries, the presence (vs. absence) of an aortic patch and the type of the arterial anastomosis (end-to-end to the hypogastric vs. end-to-side to the external iliac artery) did not have an impact on the incidence of early or late vascular complications. In kidneys with multiple arteries, only the rate of late renal artery stenosis was higher, the rate of early vascular and urologic complications was not different. Our multivariate analysis identified acute tubular necrosis as a risk factor for renal artery and vein thrombosis; graft placement on the left side for arterial thrombosis; and preservation time > or = 24 hours and multiple renal arteries for renal artery stenosis.
Results of kidney transplants using allografts with multiple versus single arteries are similar.
作者确定使用具有多条肾动脉的同种异体肾移植是否会对移植后移植物及患者的预后产生不利影响,或增加血管和泌尿系统并发症的发生率。
具有多条肾动脉的肾移植与早期血管和泌尿系统并发症的发生率增加相关。单条肾动脉与多条肾动脉的肾移植在长期移植物和患者预后、移植后高血压、急性肾小管坏死、排斥反应以及晚期血管和泌尿系统并发症的发生率方面尚未进行比较。
我们分析了1985年12月1日至1993年6月30日期间进行的998例成人肾移植,其中仅使用受体的髂外动脉或髂内动脉进行吻合。我们将研究人群分为3组:A组——1条肾动脉,1个动脉吻合口(n = 835),B组——>1条肾动脉,1个动脉吻合口(n = 112),C组——>1条肾动脉,>1个动脉吻合口(n = 51)。我们比较了移植后高血压、急性肾小管坏死、急性排斥反应以及血管和泌尿系统并发症的发生率;移植后1年、3年和5年时的平均肌酐水平;以及患者和移植物的存活率。进行单因素和多因素分析以确定血管并发症的危险因素。
我们发现三组在以下变量方面无显著差异:移植后高血压、急性肾小管坏死、急性排斥反应、肌酐水平、早期血管和泌尿系统并发症以及移植物和患者存活率。在单条肾动脉的肾脏中,主动脉补片的存在(与不存在相比)以及动脉吻合的类型(与髂内动脉端端吻合与与髂外动脉端侧吻合)对早期或晚期血管并发症的发生率没有影响。在多条肾动脉的肾脏中,仅晚期肾动脉狭窄的发生率较高,早期血管和泌尿系统并发症的发生率没有差异。我们的多因素分析确定急性肾小管坏死是肾动脉和静脉血栓形成的危险因素;移植于左侧是动脉血栓形成的危险因素;保存时间>或=24小时以及多条肾动脉是肾动脉狭窄的危险因素。
使用多条动脉与单条动脉同种异体肾移植的肾移植结果相似。