Grmec S, Gasparovic V
Emergency Medical Service, Maribor Teaching Hospital, Ljubljanska, Slovakia.
Crit Care. 2001;5(1):19-23. doi: 10.1186/cc973. Epub 2000 Dec 14.
There are numerous prehospital descriptive scoring systems, and it is uncertain whether they are efficient in assessing of the severity of illness and whether they have a prognostic role in the estimation of the illness outcome (in comparison with that of the prognostic scoring system Acute Physiology and Chronic Health Evaluation [APACHE] II). The purpose of the present study was to assess the value of the various scoring systems in predicting outcome in nontraumatic coma patients and to evaluate the importance of mental status measurement in relation to outcome.
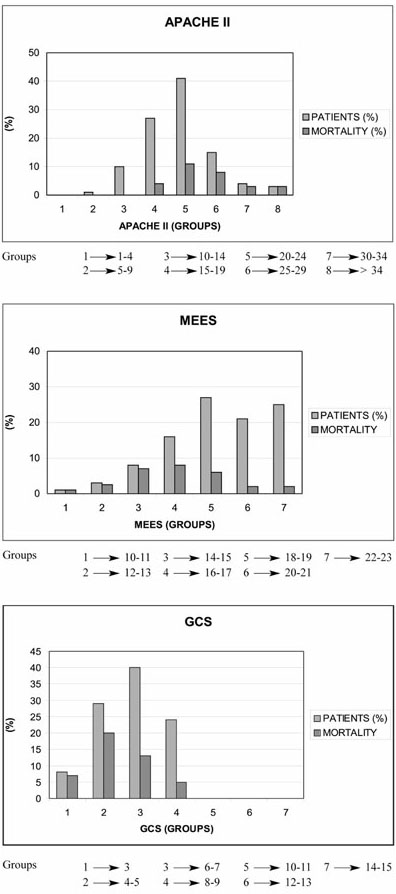
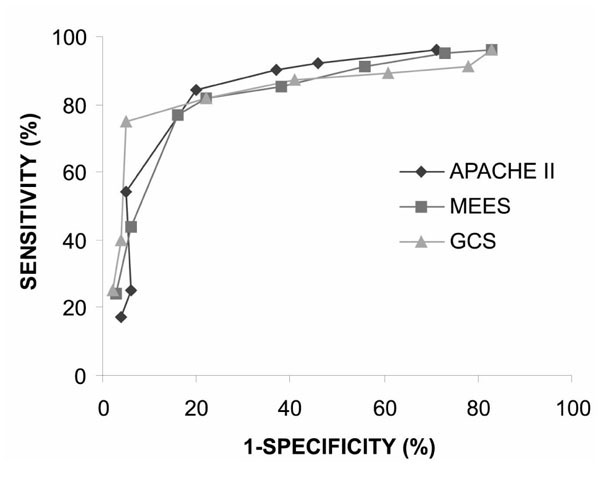
In a prehospital setting, postintervention values of the Mainz Emergency Evaluation System (MEES) and Glasgow Coma Scale (GCS) were measured for each patient. The APACHE II score was recorded on the day of admission to the hospital. This study was undertaken over a 2-year period (from January 1996 to October 1998), and included 286 consecutive patients (168 men, 118 women) who were hospitalized for nontraumatic coma. Patients younger than 16 years were not included. Their age varied from 16 to 87 years, with mean +/- standard deviation of 51.8 +/- 16.9 years. Sensitivity, specificity and correct prediction of outcome were measured using the chi2 method, with four severity scores. The best cutoff point in each scoring system was determined using the Youden index. The difference in Youden index was calculated using the Z score. For each score, the receiver operating characteristic (ROC) curve was obtained. The difference in ROC was calculated using the Z score. P < 0.05 was considered statistically significant.
For prediction of mortality, the best cutoff points were 19 for APACHE II, 18 for MEES and 5 for GCS. The best cutoffs for the Youden index were 0.63 for APACHE II, 0.61 for MEES and 0.65 for GCS. The correct prediction of outcome was achieved in 79.9% for APACHE II, 78.3% for MEES and 81.9% for GCS. The area under the ROC curve (mean +/- standard error) was 0.86 +/- 0.02 for APACHE II, 0.84 +/- 0.06 for MEES and 0.88 +/- 0.03 for GCS. There were no statistically significant differences among APACHE II, MEES and GCS scores in terms of correct prediction of outcome, Youden index or area under ROC curve.
APACHE II is not much better than prehospital descriptive scoring systems (MEES and GCS). APACHE II and MEES should not replace GCS in assessment of illness severity or in prediction of mortality in nontraumatic coma. For the assessment of mortality, the GCS score provides the best indicator for these patients (simplicity, less time-consuming and effective in an emergency situation.
有许多院前描述性评分系统,但不确定它们在评估疾病严重程度方面是否有效,以及在估计疾病预后方面是否具有预后作用(与预后评分系统急性生理与慢性健康评估[APACHE]II相比)。本研究的目的是评估各种评分系统在预测非创伤性昏迷患者预后方面的价值,并评估精神状态测量与预后的相关性。
在院前环境中,测量每位患者的美因茨急诊评估系统(MEES)和格拉斯哥昏迷量表(GCS)干预后值。在患者入院当天记录APACHE II评分。本研究为期2年(从1996年1月至1998年10月),纳入286例因非创伤性昏迷住院的连续患者(168例男性,118例女性)。不包括16岁以下患者。他们的年龄从16岁到87岁不等,平均±标准差为51.8±16.9岁。使用卡方方法,采用四个严重程度评分来测量结果的敏感性、特异性和正确预测。使用约登指数确定每个评分系统的最佳截断点。使用Z分数计算约登指数的差异。对于每个评分,获得受试者操作特征(ROC)曲线。使用Z分数计算ROC的差异。P<0.05被认为具有统计学意义。
对于死亡率预测,APACHE II的最佳截断点为19,MEES为18,GCS为5。约登指数的最佳截断值APACHE II为0.63,MEES为0.61,GCS为0.65。APACHE II对结果的正确预测率为79.9%,MEES为78.3%,GCS为81.9%。APACHE II的ROC曲线下面积(平均±标准误)为0.86±0.02,MEES为0.84±0.06,GCS为0.88±0.03。在结果的正确预测、约登指数或ROC曲线下面积方面,APACHE II、MEES和GCS评分之间无统计学显著差异。
APACHE II并不比院前描述性评分系统(MEES和GCS)好多少。在评估非创伤性昏迷的疾病严重程度或死亡率预测方面,APACHE II和MEES不应取代GCS。对于死亡率评估,GCS评分是这些患者的最佳指标(简单、耗时少且在紧急情况下有效)。