Bloomston Mark, Serafini Francesco, Boyce H Worth, Rosemurgy Alexander S
Department of Surgery, University of South Florida College of Medicine, Tampa, USA.
JSLS. 2002 Jan-Mar;6(1):41-7.
In the early 1990s, minimally invasive videoscopy was applied to numerous operations. After undertaking more than 50 "open" Heller myotomies, our experience with videoscopic Heller myotomy began in 1992. We sought to determine whether the outcome following videoscopic Heller myotomy is influenced by surgeon experience.
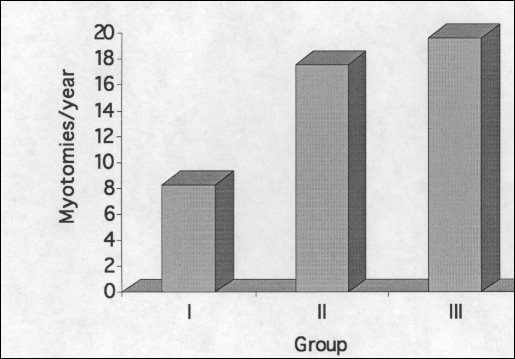
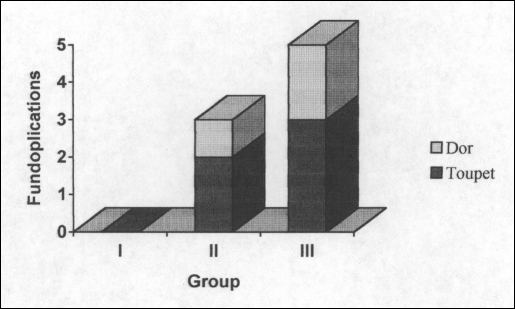
Seventy-eight patients with severe dysphagia secondary to achalasia underwent videoscopic Heller myotomy between 1992 and 1998. Intraoperative endoscopy was utilized to ensure adequate myotomy in all patients. Patients were stratified into 3 groups: the first 25 patients (group I), the second 25 patients (group II), and the last 28 patients (group III). Clinical outcome was based on length of stay, incidence of intraoperative complications, conversion to an 'open' procedure, and postoperative symptoms.
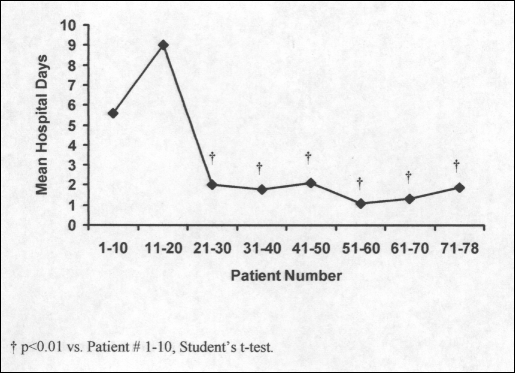
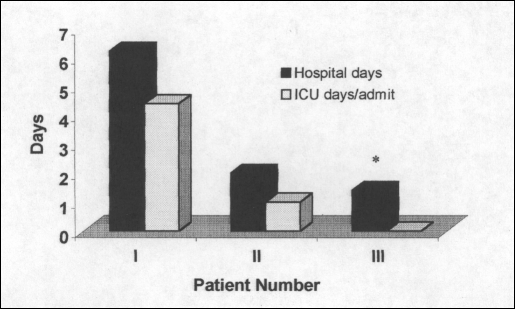
Perioperative complications occurred in 20% of patients in group I compared with 8% and 12% in groups II and III, respectively (P = NS). Only 3 patients required conversion to an 'open' procedure, all in group I (P <0 .05). Symptomatic improvement was achieved in 80% of patients in group I, 100% in group II, and 96% in group III (P < 0.05). Significant reductions in conversions to open, length of stay, and postoperative symptoms were seen after 20 myotomies were undertaken.
Outcome following videoscopic Heller myotomy, like other videoscopic operations, improves as surgeons progress along the videoscopic "learning curve." After approximately 20 videoscopic Heller myotomies, surgeons can expect fewer conversions to open procedures, shorter hospital stays, and better symptomatic relief.
20世纪90年代初,微创视频镜检查应用于众多手术。在进行了50多例“开放”的贲门肌切开术后,我们于1992年开始了视频镜下贲门肌切开术的经验。我们试图确定视频镜下贲门肌切开术的结果是否受外科医生经验的影响。
1992年至1998年间,78例因贲门失弛缓症继发严重吞咽困难的患者接受了视频镜下贲门肌切开术。术中使用内镜确保所有患者的肌切开术充分。患者被分为3组:前25例患者(I组),接下来的25例患者(II组),以及最后28例患者(III组)。临床结果基于住院时间、术中并发症发生率、转为“开放”手术的情况以及术后症状。
I组20%的患者发生围手术期并发症,而II组和III组分别为8%和12%(P = 无显著性差异)。只有3例患者需要转为“开放”手术,均在I组(P <0.05)。I组80%的患者症状改善,II组为100%,III组为96%(P <0.05)。在进行20例肌切开术后,转为开放手术的情况、住院时间和术后症状均有显著减少。
与其他视频镜手术一样,视频镜下贲门肌切开术的结果随着外科医生沿着视频镜“学习曲线”的进展而改善。在进行大约20例视频镜下贲门肌切开术后,外科医生可以预期转为开放手术的情况减少、住院时间缩短以及症状缓解更好。