Muñoz Beatriz, Solomon Anthony W, Zingeser James, Barwick Rachel, Burton Matthew, Bailey Robin, Mabey David, Foster Allen, West Sheila K
Dana Center for Preventive Ophthalmology, Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, Maryland 21287, USA.
Invest Ophthalmol Vis Sci. 2003 Apr;44(4):1464-9. doi: 10.1167/iovs.02-0234.
National programs for trachoma control are implementing mass treatment programs in which azithromycin is used as part of the control strategy. Dose is determined by weight, which can be difficult to determine in field conditions. The purposes of this study were to determine whether an accurate dose could be determined by using height as a surrogate for weight and whether a single model of height-based dosage would be applicable in more than one setting.
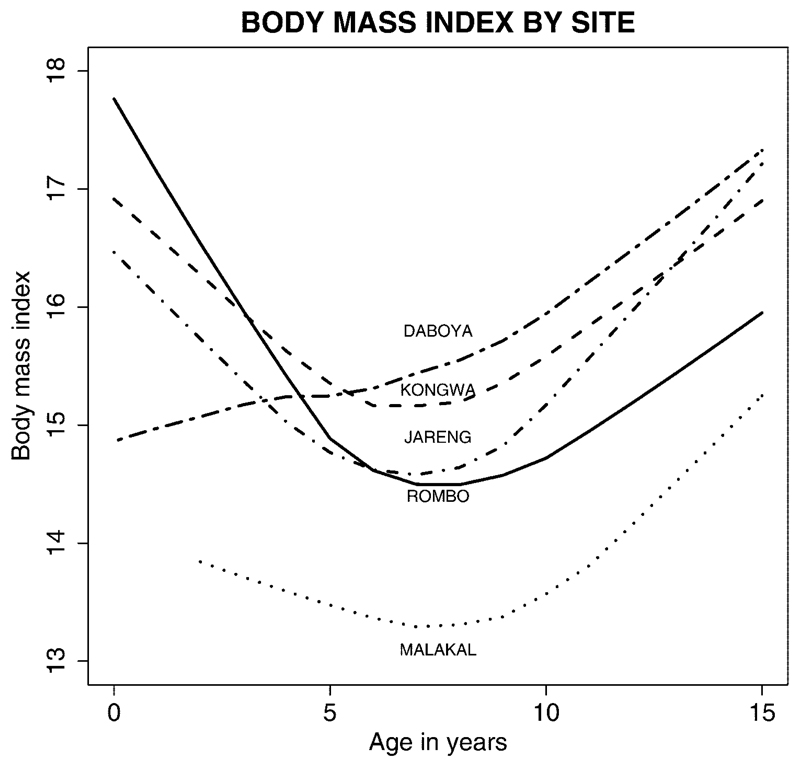
Data on height, weight, age, and gender of 5558 children aged 6 months to15 years were obtained from Kongwa and Rombo, Tanzania; Malakal, Sudan; Jareng, The Gambia; and Daboya, Ghana. Models for predicting weight by measuring height were developed that incorporated country-specific parameters. Doses of azithromycin assumed suspension of 40 mg/mL and 250-mg tablets that could be halved. Tolerance limits were defined as 15 to 30 mg/kg.
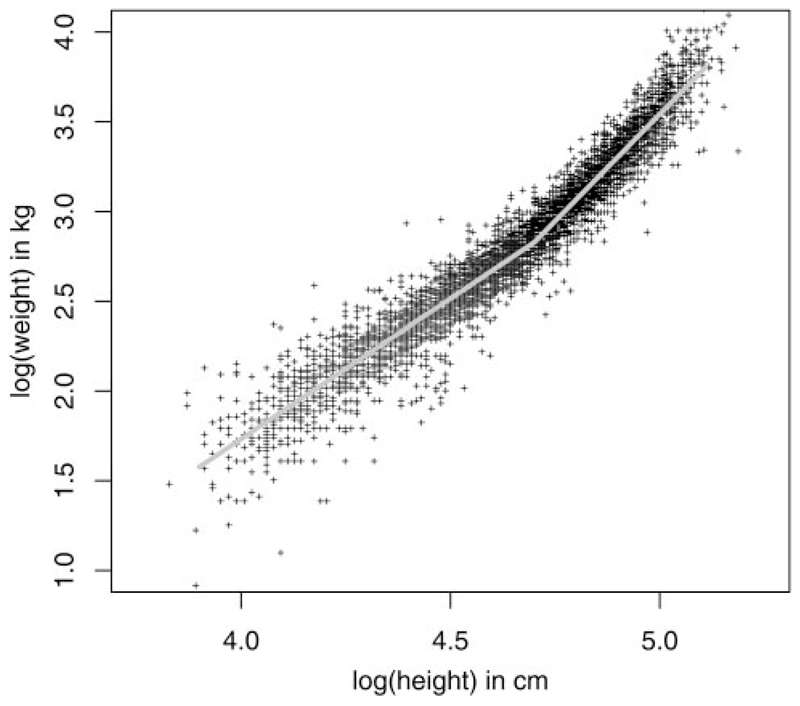
A regression model, predicting log weight as a function of log height, was the best fit and explained 94% of the variance. In children less than 1 year of age or 60 cm in height, dose determined by weight was preferred. Dosage by height resulted in more than 97% of children receiving doses within the tolerance limits. Children aged 1 to 2 years were the group most likely to be over- or undermedicated, but this occurred in only 6% of this age group.
Height-based determination of dosage of azithromycin in trachoma control programs appears to be feasible, using the height-based schedule proposed. One model was adequate for all the countries in the study. Further expansion to other countries is warranted.
国家沙眼控制项目正在实施大规模治疗项目,其中阿奇霉素被用作控制策略的一部分。剂量由体重决定,而在现场条件下体重可能难以确定。本研究的目的是确定是否可以通过使用身高作为体重的替代指标来确定准确剂量,以及基于身高的单一剂量模型是否适用于多个地区。
从坦桑尼亚的孔瓜和伦博、苏丹的马拉卡勒、冈比亚的贾伦和加纳的达博亚收集了5558名6个月至15岁儿童的身高、体重、年龄和性别的数据。开发了通过测量身高预测体重的模型,并纳入了特定国家的参数。阿奇霉素剂量假设为40mg/mL的混悬液和可分成两半的250mg片剂。耐受限度定义为15至30mg/kg。
一个将对数体重作为对数身高函数的回归模型拟合效果最佳,解释了94%的方差。对于年龄小于1岁或身高小于60cm的儿童,按体重确定剂量更为可取。按身高给药使超过97%的儿童接受的剂量在耐受限度内。1至2岁的儿童是最有可能用药过量或不足的群体,但这仅发生在该年龄组的6%。
在沙眼控制项目中,使用建议的基于身高的给药方案,基于身高确定阿奇霉素剂量似乎是可行的。一个模型适用于研究中的所有国家。有必要进一步推广到其他国家。