Schreur H J, Sterk P J, Vanderschoot J, van Klink H C, van Vollenhoven E, Dijkman J H
Department of Pulmonology, University of Leiden, The Netherlands.
Thorax. 1992 Sep;47(9):674-9. doi: 10.1136/thx.47.9.674.
A common auscultatory finding in pulmonary emphysema is a reduction of lung sounds. This might be due to a reduction in the generation of sounds due to the accompanying airflow limitation or to poor transmission of sounds due to destruction of parenchyma. Lung sound intensity was investigated in normal and emphysematous subjects in relation to airflow.
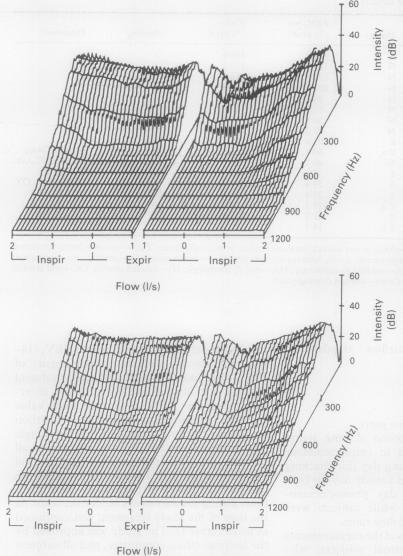
Eight normal men (45-63 years, FEV1 79-126% predicted) and nine men with severe emphysema (50-70 years, FEV1 14-63% predicted) participated in the study. Emphysema was diagnosed according to pulmonary history, results of lung function tests, and radiographic criteria. All subjects underwent phonopneumography during standardised breathing manoeuvres between 0.5 and 2 1 below total lung capacity with inspiratory and expiratory target airflows of 2 and 1 l/s respectively during 50 seconds. The synchronous measurements included airflow at the mouth and lung volume changes, and lung sounds at four locations on the right chest wall. For each microphone airflow dependent power spectra were computed by using fast Fourier transformation. Lung sound intensity was expressed as log power (in dB) at 200 Hz at inspiratory flow rates of 1 and 2 l/s and at an expiratory flow rate of 1 l/s.
Lung sound intensity was well repeatable on two separate days, the intraclass correlation coefficient ranging from 0.77 to 0.94 between the four microphones. The intensity was strongly influenced by microphone location and airflow. There was, however, no significant difference in lung sound intensity at any flow rate between the normal and the emphysema group.
Airflow standardised lung sound intensity does not differ between normal and emphysematous subjects. This suggests that the auscultatory finding of diminished breath sounds during the regular physical examination in patients with emphysema is due predominantly to airflow limitation.
肺气肿常见的听诊表现是肺音减弱。这可能是由于伴随的气流受限导致声音产生减少,或者是由于实质破坏导致声音传导不良。研究了正常人和肺气肿患者的肺音强度与气流的关系。
8名正常男性(45 - 63岁,FEV1为预测值的79 - 126%)和9名重度肺气肿男性(50 - 70岁,FEV1为预测值的14 - 63%)参与了研究。根据肺部病史、肺功能测试结果和影像学标准诊断肺气肿。所有受试者在肺总量以下0.5至2升的标准化呼吸动作期间进行呼吸音描记,在50秒内吸气和呼气目标气流分别为2升/秒和1升/秒。同步测量包括口腔气流、肺容积变化以及右胸壁四个位置的肺音。对于每个麦克风,通过快速傅里叶变换计算气流相关的功率谱。肺音强度表示为在吸气流量1升/秒和2升/秒以及呼气流量1升/秒时200赫兹处的对数功率(以分贝为单位)。
肺音强度在两个不同日期具有良好的可重复性,四个麦克风之间的组内相关系数在0.77至0.94之间。强度受麦克风位置和气流的强烈影响。然而,正常组和肺气肿组在任何流速下的肺音强度均无显著差异。
正常人和肺气肿患者在气流标准化的情况下肺音强度没有差异。这表明肺气肿患者在常规体格检查中呼吸音减弱的听诊表现主要是由于气流受限。