von Dossow Vera, Schilling Corinna, Beller Stefan, Hein Ortrud Vargas, von Heymann Christian, Kox Wolfgang J, Spies Claudia D
Department of Anesthesiology and Intensive Care Medicine, Charité - Universitätsmedizin Berlin, Berlin, Germany.
Crit Care. 2004 Oct;8(5):R312-21. doi: 10.1186/cc2911. Epub 2004 Jul 20.
Chronic alcoholic patients have a threefold to fourfold increased risk for developing a severe infection or septic shock after surgery, which might be due to altered immune response. The aim of this outcome matched study was to investigate proinflammatory and anti-inflammatory immune parameters during the course of infection and subsequent septic shock in chronic alcoholic patients, and to compare these parameters with those in nonalcoholic patients.
Twenty-eight patients from a cohort of fifty-six with either pneumonia or peritonitis and subsequent septic shock were selected. Fourteen patients were chronic alcoholics whereas fourteen were nonalcoholic patients. Chronic alcoholic patients met criteria (Diagnostic and Statistical Manual of Mental Disorders IV, of the American Psychiatric Association) for alcohol abuse or dependence. Measurements were performed during the onset of infection (within 24 hours after the onset of infection), in early septic shock (within 12 hours after onset of septic shock) and in late septic shock (72 hours after the onset). Blood measurements included proinflammatory and anti-inflammatory cytokines.
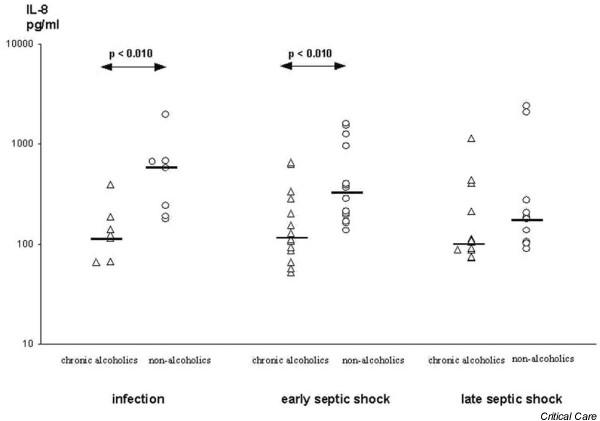
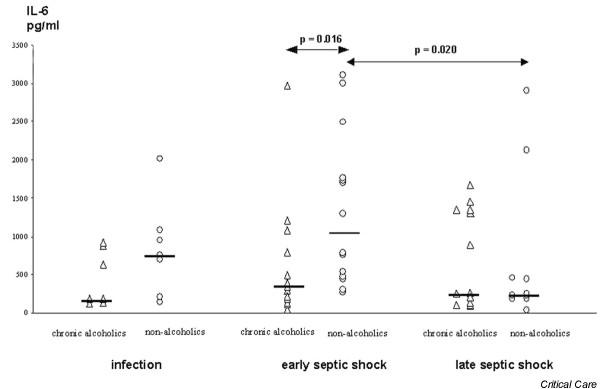
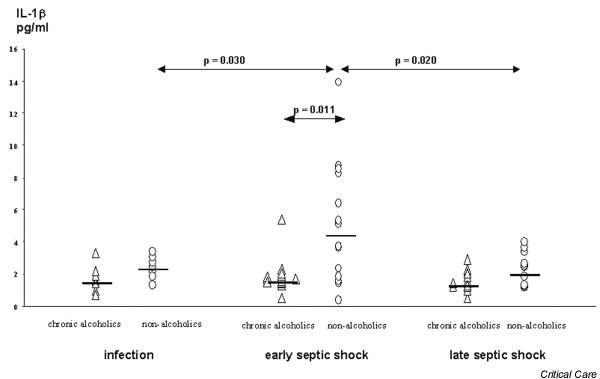
Chronic alcoholic patients exhibited significantly lower plasma levels of IL-8 (P < 0.010) during the onset of infection than did matched nonalcoholic patients. In early septic shock, chronic alcoholic patients had significantly decreased levels of IL-1beta (P < 0.015), IL-6 (P < 0.016) and IL-8 (P < 0.010). The anti-inflammatory parameters IL-10 and tumour necrosis factor receptors I and II did not differ between alcoholic and nonalcoholic patients.
At the onset of infection and during early septic shock, chronic alcoholic patients had lower levels of proinflammatory immune parameters than did nonalcoholic patients. Therefore, immunomodulatory therapy administered early may be considered in chronic alcoholic patients at the onset of an infection because of their altered proinflammatory immune response.
慢性酒精性患者术后发生严重感染或感染性休克的风险增加三到四倍,这可能归因于免疫反应改变。本结果匹配研究的目的是调查慢性酒精性患者在感染及随后的感染性休克过程中的促炎和抗炎免疫参数,并将这些参数与非酒精性患者的参数进行比较。
从56例患有肺炎或腹膜炎并随后发生感染性休克的队列中选择28例患者。14例为慢性酒精性患者,14例为非酒精性患者。慢性酒精性患者符合美国精神病学协会《精神疾病诊断与统计手册》第四版中酒精滥用或依赖的标准。在感染发作时(感染发作后24小时内)、感染性休克早期(感染性休克发作后12小时内)和感染性休克晚期(发作后72小时)进行测量。血液检测包括促炎和抗炎细胞因子。
在感染发作时,慢性酒精性患者的血浆IL-8水平显著低于匹配的非酒精性患者(P < 0.010)。在感染性休克早期,慢性酒精性患者的IL-1β(P < 0.015)、IL-6(P < 0.016)和IL-8(P < 0.010)水平显著降低。酒精性和非酒精性患者之间的抗炎参数IL-10以及肿瘤坏死因子受体I和II没有差异。
在感染发作时和感染性休克早期,慢性酒精性患者的促炎免疫参数水平低于非酒精性患者。因此,由于慢性酒精性患者促炎免疫反应改变,在感染发作时可考虑对其进行早期免疫调节治疗。