Hallas Peter, Ellingsen Trond
Department of Surgery, Hålogalandssykehuset Harstad, 9406 Harstad, Norway.
BMC Emerg Med. 2006 Feb 16;6:4. doi: 10.1186/1471-227X-6-4.
Evaluation of the circumstances related to errors in diagnosis of fractures at an Emergency Department may suggest ways to reduce the incidence of such errors.
Retrospective analysis of all cases during a two year period (2002-2004) where a fracture had been overlooked or an injury had been erroneously diagnosed as a fracture (n = 61). 100 random selected patients with correctly diagnosed fractures served as control group.
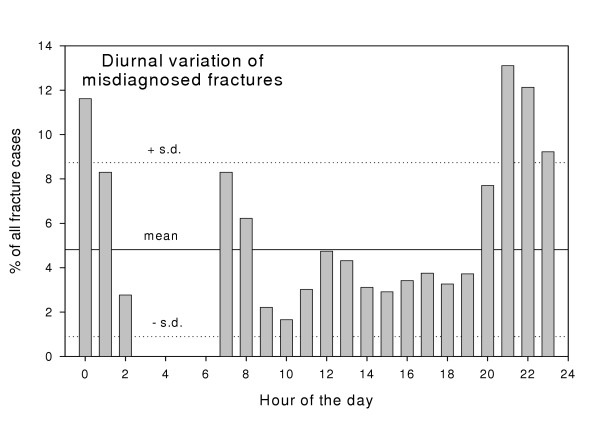
In the two year period 5879 patients visited the ED with injuries. 1% of all visits to the ED resulted in an error in fracture diagnosis and 3.1% of all fractures were not diagnosed at the initial visit to the ED. 86% of such errors had consequences for treatment. No patient characteristics could be identified as risk factors for a misdiagnosis of a fracture. There was a peak in errors in fracture diagnoses between 8 pm and 2 am (47% against 20% in controls, p < 0.005).
A considerable number of fractures were not correctly diagnosed at the initial ED visit. There was a diurnal variation in the rate of misdiagnosis of fractures with a significant peak from 8 pm to 2 am. Where there was an error in fracture diagnosis, the patients did not appear to have a characteristic profile as regarding e.g. age, sex or capability to communicate with the ED staff. Increased consultancy service in radiology may reduce the frequency of errors in diagnosis, particularly in the evenings between 8 pm and 2 am.
对急诊科骨折诊断错误相关情况的评估可能会提示减少此类错误发生率的方法。
对两年期间(2002 - 2004年)所有骨折被漏诊或损伤被误诊为骨折的病例(n = 61)进行回顾性分析。随机选择100例骨折诊断正确的患者作为对照组。
在这两年期间,有5879名受伤患者到急诊科就诊。急诊科所有就诊病例中1%导致骨折诊断错误,所有骨折病例中3.1%在首次到急诊科就诊时未被诊断出来。此类错误中有86%对治疗产生了影响。未发现任何患者特征可作为骨折误诊的危险因素。晚上8点至凌晨2点之间骨折诊断错误出现高峰(47%,而对照组为20%,p < 0.005)。
相当数量的骨折在首次到急诊科就诊时未得到正确诊断。骨折误诊率存在日变化,晚上8点至凌晨2点有显著高峰。在骨折诊断出现错误的情况下,患者在年龄、性别或与急诊科工作人员沟通能力等方面似乎没有特征性表现。增加放射科会诊服务可能会降低诊断错误的频率,尤其是在晚上8点至凌晨2点之间。