Gummesson Christina, Ward Michael M, Atroshi Isam
National Institute of Arthritis and Musculoskeletal and Skin Diseases, NIH, Bethesda, Maryland 20892, USA.
BMC Musculoskelet Disord. 2006 May 18;7:44. doi: 10.1186/1471-2474-7-44.
The 30-item disabilities of the arm, shoulder and hand (DASH) questionnaire is increasingly used in clinical research involving upper extremity musculoskeletal disorders. From the original DASH a shorter version, the 11-item QuickDASH, has been developed. Little is known about the discriminant ability of score changes for the QuickDASH compared to the DASH. The aim of this study was to assess the performance of the QuickDASH and its cross-sectional and longitudinal validity and reliability.
The study was based on extracting QuickDASH item responses from the responses to the full-length DASH questionnaire completed by 105 patients with a variety of upper extremity disorders before surgery and at follow-up 6 to 21 months after surgery. The DASH and QuickDASH scores were compared for the whole population and for different diagnostic groups. For longitudinal construct validity the effect size and standardized response mean were calculated. Analyses with ROC curves were performed to compare the ability of the DASH and QuickDASH to discriminate among patients classified according to the magnitude of self-rated improvement. Cross-sectional and test-retest reliability was assessed.
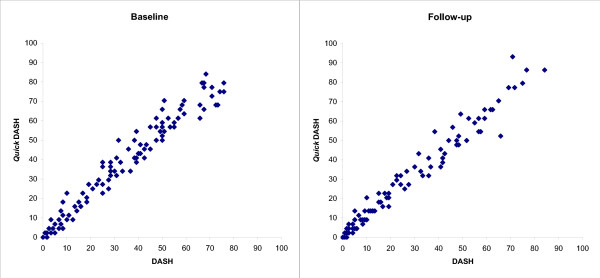
The mean DASH score was 34 (SD 22) and the mean QuickDASH score was 39 (SD 24) at baseline. For the different diagnostic groups the mean and median QuickDASH scores were higher than the corresponding DASH scores. For the whole population, the mean difference between the QuickDASH and DASH baseline scores was 4.2 (95% CI 3.2-5.3), follow-up scores was 2.6 (1.7-3.4), and change scores was 1.7 (0.6-2.8). The overall effect size and standardized response mean measured with the DASH and the QuickDASH were similar. In the ROC analysis of change scores among patients who rated their arm status as somewhat or much better and those who rated it as unchanged the difference in the area under the ROC curve for the DASH and QuickDASH was 0.01 (95% CI -0.05-0.07) indicating similar discriminant ability.Cross-sectional and test-retest reliability of the DASH and QuickDASH were similar.
The results indicate that the QuickDASH can be used instead of the DASH with similar precision in upper extremity disorders.
30项上肢、肩部和手部功能障碍(DASH)问卷在涉及上肢肌肉骨骼疾病的临床研究中使用得越来越多。在原始DASH基础上开发了一个更简短的版本,即11项快速DASH(QuickDASH)。与DASH相比,关于QuickDASH评分变化的判别能力知之甚少。本研究的目的是评估QuickDASH的性能及其横断面和纵向效度与信度。
本研究基于从105例患有各种上肢疾病的患者术前及术后6至21个月随访时填写的全长DASH问卷的回答中提取QuickDASH项目的回答。比较了整个人群以及不同诊断组的DASH和QuickDASH评分。对于纵向结构效度,计算了效应量和标准化反应均值。进行ROC曲线分析以比较DASH和QuickDASH区分根据自我评定改善程度分类的患者的能力。评估了横断面信度和重测信度。
基线时DASH平均评分为34(标准差22),QuickDASH平均评分为39(标准差24)。对于不同诊断组,QuickDASH的平均和中位数评分高于相应的DASH评分。对于整个人群,QuickDASH与DASH基线评分的平均差异为4.2(95%CI 3.2 - 5.3),随访评分为2.6(1.7 - 3.4),变化评分为1.7(0.6 - 2.8)。用DASH和QuickDASH测量的总体效应量和标准化反应均值相似。在对将手臂状况评为有所改善或明显改善及评为无变化的患者的变化评分进行的ROC分析中,DASH和QuickDASH的ROC曲线下面积差异为0.01(95%CI -0.05 - 0.07),表明判别能力相似。DASH和QuickDASH的横断面信度和重测信度相似。
结果表明,在评估上肢疾病时,QuickDASH可以替代DASH,且具有相似的精度。