Shorr Andrew F, Bernard Gordon R, Dhainaut Jean-Francois, Russell James R, Macias William L, Nelson David R, Sundin David P
Department of Medicine, Section of Pulmonary and Critical Care Medicine, Washington Hospital Center, Washington, DC, USA.
Crit Care. 2006;10(3):R92. doi: 10.1186/cc4946. Epub 2006 Jun 15.
Protein C, because of its central role in hemostasis, plays an integral role in the host response to infection. Protein C depletion, resulting from increased consumption, degradation, and/or decreased synthesis, is characteristic of sepsis and has been shown to predict morbidity and mortality. The objective of this study was to determine whether early directional changes in protein C levels correlate with outcome.
Patients in the Recombinant Human Activated Protein C Worldwide Evaluation in Severe Sepsis (PROWESS) clinical trial were assessed and categorized by baseline protein C (n = 1574). Deficiency was categorized as: severe deficiency, protein C levels < or = 40% of normal protein C activity (n = 615, 39% of patients); deficient, protein C levels 41-80% of normal protein C activity (n = 764, 48.5% of patients); and normal, >80% of normal protein C activity (n = 195, 12.4% of patients). Logistic regression analysis of 28-day mortality for placebo patients was used to investigate whether baseline and day 1 protein C levels were independent risk factors for mortality. The impact of treatment with drotrecogin alfa (activated) (DrotAA) was also assessed.
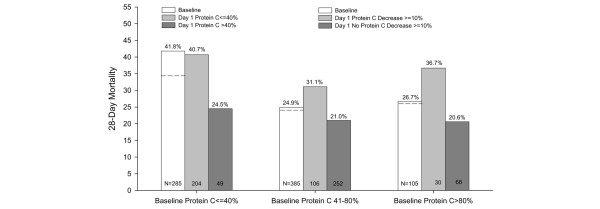
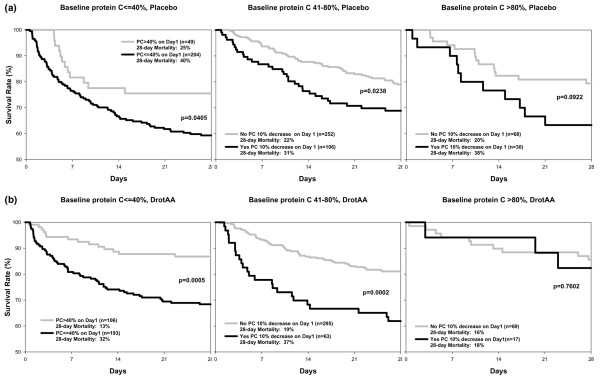
Protein C levels at baseline and day 1 were independent risk factors in placebo patients. If baseline protein C levels of severely deficient placebo patients remained < or = 40% at day 1 their odds of death increased (odds ratio = 2.75, P < 0.0001), while if levels improved to >40% by day 1 their risk of death decreased (odds ratio = 0.43, P = 0.03). If baseline protein C levels of placebo patients were >40% but decreased by > or = 10% on day 1, their risk of death increased (odds ratio = 1.87, P = 0.02). DrotAA treatment improved protein C levels by day 1 compared with placebo (P = 0.008) and reduced the risk of death in severely deficient (< or = 40%) patients at baseline. Treatment also decreased the number of severely protein C deficient (= 40%) patients and decreased the number of deficient (41-80%) patients and normal (>80%) patients who had a > or = 10% decrease in protein C levels by day 1.
Baseline protein C levels were an independent predictor of sepsis outcome. Day 1 changes in protein C, regardless of baseline levels, were also predictive of outcome. The association of DrotAA treatment, increased protein C levels, and improved survival may partially explain the mechanism of action.
蛋白C因其在止血过程中的核心作用,在宿主对感染的反应中发挥着不可或缺的作用。由于消耗增加、降解以及/或合成减少导致的蛋白C水平降低,是脓毒症的特征,并且已被证明可预测发病率和死亡率。本研究的目的是确定蛋白C水平的早期方向性变化是否与预后相关。
对严重脓毒症重组人活化蛋白C全球评估(PROWESS)临床试验中的患者进行评估,并根据基线蛋白C水平(n = 1574)进行分类。缺乏被分为:严重缺乏,蛋白C水平低于或等于正常蛋白C活性的40%(n = 615,占患者的39%);缺乏,蛋白C水平为正常蛋白C活性的41 - 80%(n = 764,占患者的48.5%);以及正常,蛋白C活性高于正常的80%(n = 195,占患者的12.4%)。使用安慰剂患者28天死亡率的逻辑回归分析来研究基线和第1天的蛋白C水平是否为死亡率的独立危险因素。还评估了重组人活化蛋白C(DrotAA)治疗的影响。
基线和第1天的蛋白C水平是安慰剂患者的独立危险因素。如果严重缺乏的安慰剂患者的基线蛋白C水平在第1天仍低于或等于40%,其死亡几率增加(比值比 = 2.75,P < 0.0001),而如果到第1天水平提高到>40%,其死亡风险降低(比值比 = 0.43,P = 0.03)。如果安慰剂患者的基线蛋白C水平>40%但在第1天下降了>或 = 10%,其死亡风险增加(比值比 = 1.87,P = 0.02)。与安慰剂相比,DrotAA治疗在第1天时改善了蛋白C水平(P = 0.008),并降低了基线时严重缺乏(<或 = 40%)患者的死亡风险。治疗还减少了严重蛋白C缺乏(= 40%)患者的数量,以及第1天蛋白C水平下降>或 = 10%的缺乏(41 - 80%)患者和正常(>80%)患者的数量。
基线蛋白C水平是脓毒症预后的独立预测指标。无论基线水平如何,第1天蛋白C的变化也可预测预后。DrotAA治疗、蛋白C水平升高与生存率改善之间的关联可能部分解释了其作用机制。