Ahmed Ali, Perry Gilbert J, Fleg Jerome L, Love Thomas E, Goff David C, Kitzman Dalane W
University of Alabama at Birmingham and VA Medical Center, Birmingham, AL 35294-2041, USA.
Am Heart J. 2006 Nov;152(5):956-66. doi: 10.1016/j.ahj.2006.06.020.
Prior studies demonstrating significant difference in outcomes in systolic and diastolic heart failure (HF) are often limited to hospitalized acute HF patients, and may be confounded by residual bias. In this analysis, we examined long-term mortality and hospitalization in a propensity score matched cohort of ambulatory chronic systolic and diastolic HF patients.
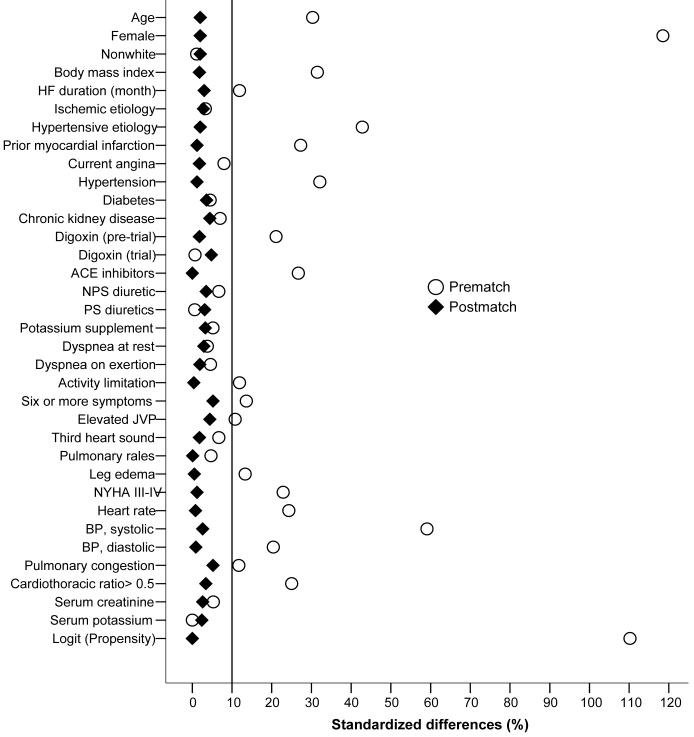
Of the 7788 patients in the Digitalis Investigation Group trial, 6800 had systolic HF (ejection fraction >45%) and 988 had diastolic HF (ejection fraction >45%). We restricted our analysis to 7617 patients without valvular heart disease: 916 diastolic HF and 6701 systolic HF. Propensity scores for diastolic HF, calculated for each patient by a non-parsimonious multivariable logistic regression model, were used to match 697 diastolic HF with 2091 systolic HF patients. Matched Cox regression models were used to estimate hazard ratios (HR) and 95% confidence intervals (CI) for outcomes in diastolic (versus systolic) HF.
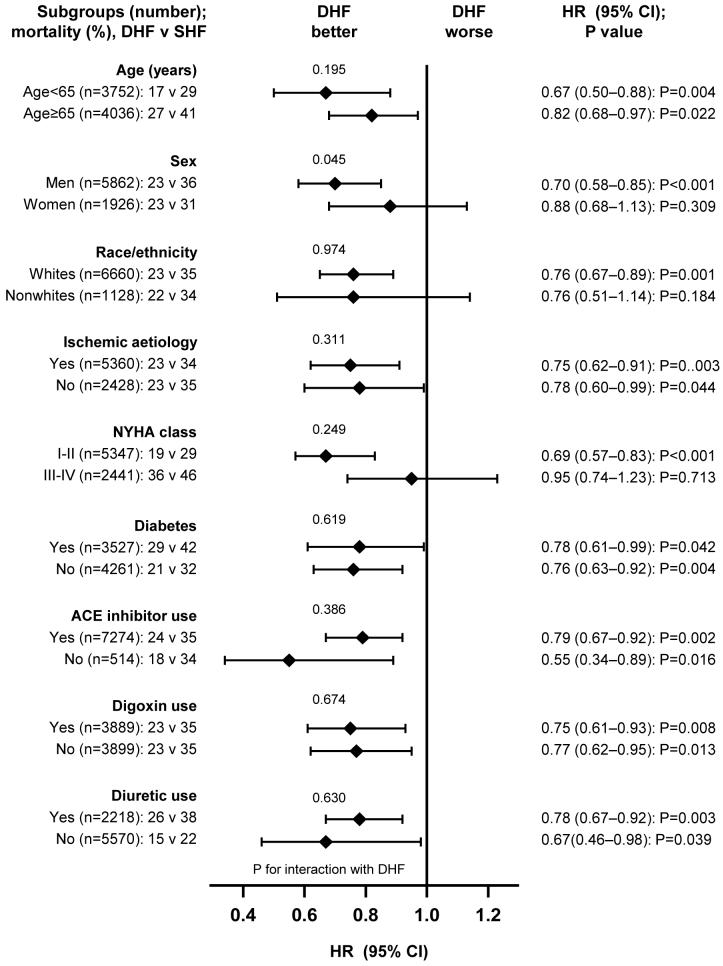
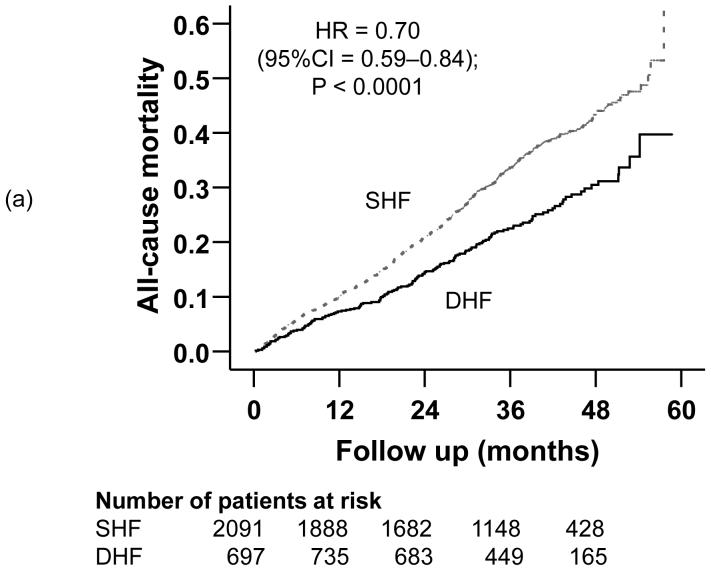
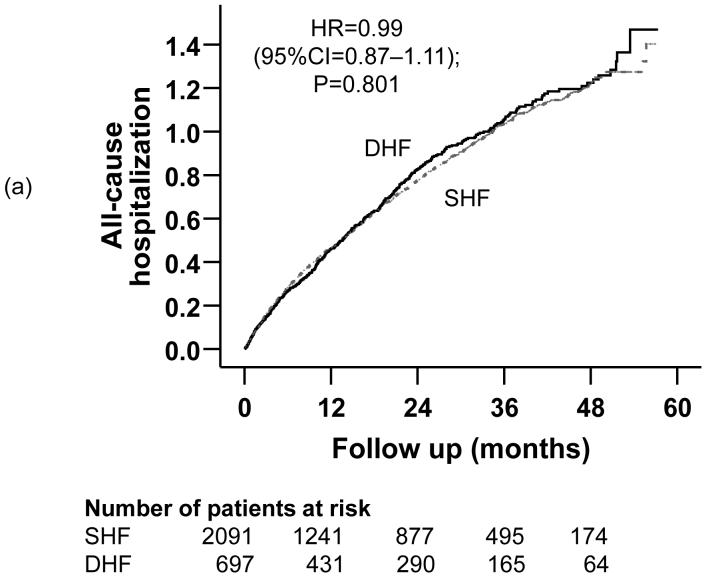
During a median 38-month follow-up, compared with 32% mortality in systolic HF, 23% of diastolic HF patients died (HR=0.70; 95% CI=0.59-0.84; P<.0001). Respective HR (95%CI) for cardiovascular and HF mortality were 0.60 (0.48-0.74; P<.0001) and 0.56 (0.39-0.79; P=.001). All-cause hospitalizations occurred in 64% of systolic and 67% of diastolic HF patients (HR=0.99; 95% CI=0.87-1.11; P=0.801). Respective HR (95%CI) for cardiovascular and HF hospitalizations were 0.84 (0.73-0.96; P=.011) and 0.63 (0.51-0.77; P<.0001).
Despite lower mortality and cardiovascular morbidity, diastolic HF patients had similar overall hospitalizations as in systolic HF. Ejection fraction should be assessed in all HF patients to guide therapy, with special attention to non-cardiovascular morbidity in diastolic HF.
先前的研究表明收缩性和舒张性心力衰竭(HF)的预后存在显著差异,但这些研究通常仅限于住院的急性HF患者,并且可能存在残余偏倚的干扰。在本分析中,我们在一个倾向评分匹配队列中研究了门诊慢性收缩性和舒张性HF患者的长期死亡率和住院情况。
在洋地黄研究组试验的7788例患者中,6800例为收缩性HF(射血分数>45%),988例为舒张性HF(射血分数>45%)。我们将分析限制在7617例无瓣膜性心脏病的患者:916例舒张性HF和6701例收缩性HF。通过非简约多变量逻辑回归模型为每位患者计算舒张性HF的倾向评分,用于将697例舒张性HF患者与2091例收缩性HF患者进行匹配。使用匹配的Cox回归模型估计舒张性(与收缩性)HF患者预后的风险比(HR)和95%置信区间(CI)。
在中位38个月的随访期间,与收缩性HF患者32%的死亡率相比,舒张性HF患者的死亡率为23%(HR=0.70;95%CI=0.59-0.84;P<0.0001)。心血管疾病和HF死亡率的HR(95%CI)分别为0.60(0.48-0.74;P<0.0001)和0.56(0.39-0.79;P=0.001)。64%的收缩性HF患者和67%的舒张性HF患者发生了全因住院(HR=0.99;95%CI=0.87-1.11;P=0.801)。心血管疾病和HF住院的HR(95%CI)分别为0.84(0.73-0.96;P=0.011)和0.63(0.51-0.77;P<0.0001)。
尽管舒张性HF患者的死亡率和心血管发病率较低,但其总体住院情况与收缩性HF患者相似。应评估所有HF患者的射血分数以指导治疗,特别关注舒张性HF患者的非心血管疾病发病率。