Ix Joachim H, Shlipak Michael G, Chertow Glenn M, Whooley Mary A
Division of Nephrology, Department of Medicine, Box 0532, HSE 672, University of California at San Francisco, San Francisco, CA 94143-0532, USA.
Circulation. 2007 Jan 16;115(2):173-9. doi: 10.1161/CIRCULATIONAHA.106.644286. Epub 2006 Dec 26.
Serum creatinine and related estimating equations predict cardiovascular events and mortality among persons with coronary heart disease (CHD). Cystatin C is a novel and sensitive endogenous marker of kidney function. Whether cystatin C concentrations are associated with adverse events among ambulatory persons with CHD is unknown.
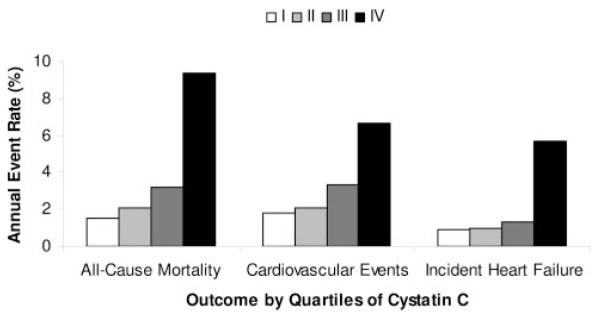
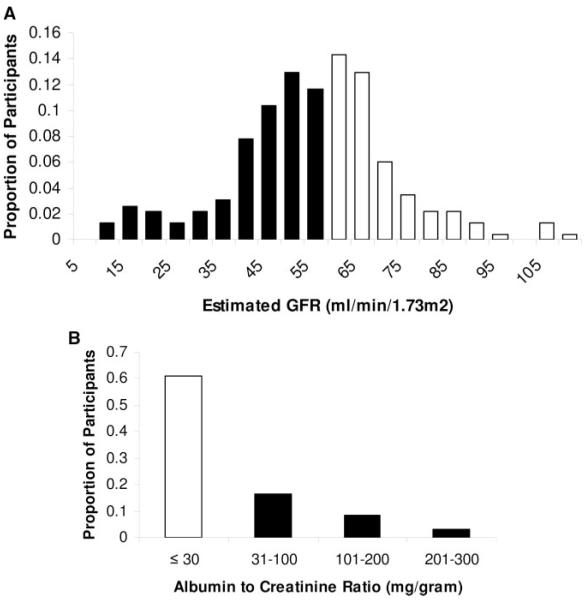
Nine hundred ninety ambulatory persons with CHD were categorized into quartiles of serum cystatin C at inception, with < or = 0.91 mg/L constituting the lowest quartile (I) and > or = 1.30 mg/L constituting the highest (IV). Cox proportional hazards models evaluated time to all-cause mortality, cardiovascular events (composite of CHD death, myocardial infarction, and stroke), and incident heart failure. After a median follow-up of 37 months, 132 participants (13%) died, 101 (10%) had cardiovascular events, and 57 (7%) had incident heart failure. Compared with participants in the lowest cystatin C quartile, those in the highest quartile were at increased risk of all-cause mortality (hazard ratio, 3.6; 95% CI, 1.8 to 7.0), cardiovascular events (hazard ratio, 2.0; 95% CI, 1.0 to 3.8), and incident heart failure (hazard ratio, 2.6; 95% CI, 1.0 to 6.9) in analyses adjusted for traditional cardiovascular risk factors. Cystatin C in the highest quartile predicted similar risk for these outcomes among participants with lower (< or = 60 mL/min per 1.73 m2) or higher estimated glomerular filtration rate and among participants with or without microalbuminuria.
High cystatin C concentrations predict substantial increased risks of all-cause mortality, cardiovascular events, and incident heart failure among ambulatory persons with CHD. This risk is not completely captured by measures of kidney function routinely used in clinical practice.
血清肌酐及相关估算方程可预测冠心病(CHD)患者的心血管事件和死亡率。胱抑素C是一种新型且敏感的肾功能内源性标志物。CHD门诊患者的胱抑素C浓度是否与不良事件相关尚不清楚。
990例CHD门诊患者在入组时被分为血清胱抑素C四分位数组,血清胱抑素C≤0.91mg/L为最低四分位数组(I组),≥1.30mg/L为最高四分位数组(IV组)。Cox比例风险模型评估全因死亡率、心血管事件(CHD死亡、心肌梗死和中风的复合事件)和新发心力衰竭的发生时间。中位随访37个月后,132例参与者(13%)死亡,101例(10%)发生心血管事件,57例(7%)出现新发心力衰竭。在对传统心血管危险因素进行校正的分析中,与胱抑素C最低四分位数组的参与者相比,最高四分位数组的参与者全因死亡率(风险比,3.6;95%CI,1.8至7.0)、心血管事件(风险比,2.0;95%CI,1.0至3.8)和新发心力衰竭(风险比,2.6;95%CI,1.0至6.9)的风险增加。最高四分位数组的胱抑素C在估算肾小球滤过率较低(≤60ml/min/1.73m²)或较高的参与者以及有或无微白蛋白尿的参与者中,对这些结局的预测风险相似。
高胱抑素C浓度可预测CHD门诊患者全因死亡率、心血管事件和新发心力衰竭的风险大幅增加。这种风险在临床实践中常规使用的肾功能测量指标中并未完全体现。