Agarwal Shradha, Cunningham-Rundles Charlotte
Division of Clinical Immunology, Mount Sinai School of Medicine, New York, New York 10029, USA.
Ann Allergy Asthma Immunol. 2007 Feb;98(2):185-90. doi: 10.1016/S1081-1206(10)60695-3.
Good syndrome is a rare cause of combined B- and T-cell immunodeficiency that occurs in association with a thymoma. Patients affected with Good syndrome have increased susceptibility to bacterial, fungal, viral, and opportunistic infections.
To describe 2 unusual cases of infections in patients with Good syndrome and review the literature.
Case 1 describes a 51-year-old woman with Good syndrome who presented with a 10-day history of diarrhea, nausea, and fevers. During her hospitalization she became pancytopenic and underwent a bone marrow biopsy and evaluation of her peripheral blood smear. Case 2 describes an 89-year-old man with Good syndrome who presented with a nonhealing leg ulcer, which underwent biopsy. A literature search through MEDLINE was performed. Keywords included Good syndrome, thymoma, hypogammaglobulinemia, immunodeficiency, and infection.
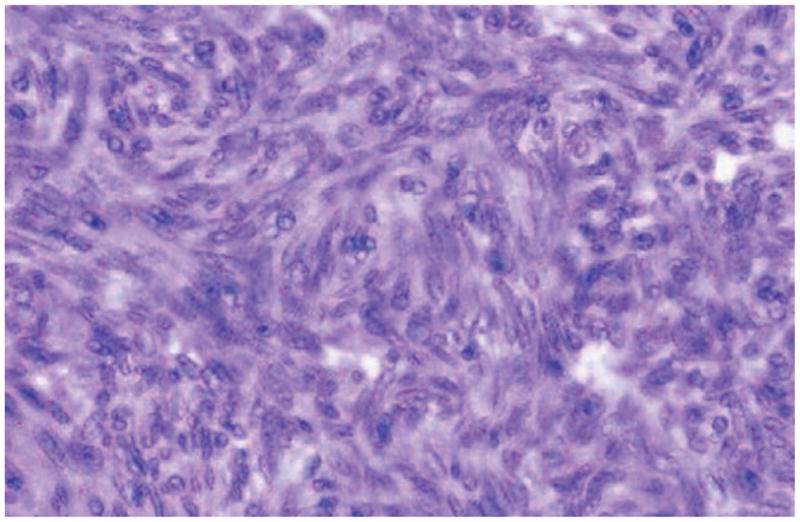
The peripheral blood smear in patient 1 showed ring-formed parasites in red blood cells suggestive of babesiosis. She began treatment with azithromycin, atovaquone, and doxycycline and recovered completely. Patient 2 underwent a biopsy of the foot. Immunohistochemical staining was positive for human herpesvirus 8 consistent with Kaposi sarcoma.
The concomitant occurrence of immunodeficiency and thymoma is known as Good syndrome. In contrast to other humoral immune defects, patients with this syndrome can develop opportunistic infections, and the prognosis appears less favorable compared with X-linked agammaglobulinemia or common variable immunodeficiency. Immunological investigations, including T-cell subsets, B cells, and quantitative immunoglobulins, should be considered part of the routine diagnostic evaluation in patients with a thymoma and recurrent infections.
古德综合征是一种罕见的B细胞和T细胞联合免疫缺陷病因,与胸腺瘤相关。患有古德综合征的患者对细菌、真菌、病毒和机会性感染的易感性增加。
描述2例古德综合征患者的不寻常感染病例并复习相关文献。
病例1描述了一名51岁患有古德综合征的女性,有10天的腹泻、恶心和发热病史。住院期间她出现全血细胞减少,并接受了骨髓活检和外周血涂片评估。病例2描述了一名89岁患有古德综合征的男性,有一个不愈合的腿部溃疡,该溃疡接受了活检。通过医学期刊数据库进行了文献检索。关键词包括古德综合征、胸腺瘤、低丙种球蛋白血症、免疫缺陷和感染。
患者1的外周血涂片显示红细胞中有环形寄生虫,提示巴贝斯虫病。她开始使用阿奇霉素、阿托伐醌和强力霉素治疗,并完全康复。患者2接受了足部活检。免疫组织化学染色显示人类疱疹病毒8呈阳性,符合卡波西肉瘤。
免疫缺陷与胸腺瘤同时出现被称为古德综合征。与其他体液免疫缺陷不同,该综合征患者可发生机会性感染,与X连锁无丙种球蛋白血症或常见变异型免疫缺陷相比,预后似乎较差。对于患有胸腺瘤和反复感染的患者,免疫学检查,包括T细胞亚群、B细胞和定量免疫球蛋白,应被视为常规诊断评估的一部分。