International Centre for Eye Health, London School of Hygiene & Tropical Medicine, London, UK
School of Optometry and Vision Science, Faculty of Medicine and Health Sciences, The University of Auckland, Auckland, New Zealand.
BMJ Glob Health. 2021 Mar;6(3). doi: 10.1136/bmjgh-2020-004484.
Globally, there are ~370 million Indigenous peoples. Indigenous peoples typically experience worse health compared with non-Indigenous people, including higher rates of avoidable vision impairment. Much of this gap in eye health can be attributed to barriers that impede access to eye care services. We conducted a scoping review to identify and summarise service delivery models designed to improve access to eye care for Indigenous peoples in high-income countries.
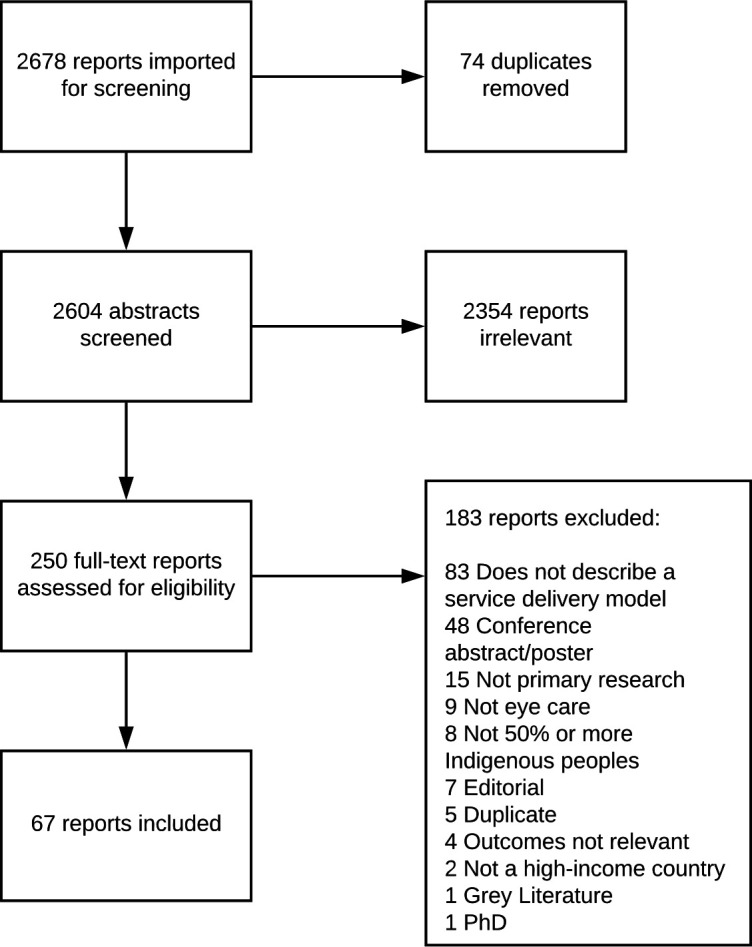
Searches were conducted on MEDLINE, Embase and Global Health in January 2019 and updated in July 2020. All study designs were eligible if they described a model of eye care service delivery aimed at populations with over 50% Indigenous peoples. Two reviewers independently screened titles, abstracts and full-text articles and completed data charting. We extracted data on publication details, study context, service delivery interventions, outcomes and evaluations, engagement with Indigenous peoples and access dimensions targeted. We summarised findings descriptively following thematic analysis.
We screened 2604 abstracts and 67 studies fulfilled our eligibility criteria. Studies were focused on Indigenous peoples in Australia (n=45), USA (n=11), Canada (n=7), New Zealand (n=2), Taiwan (n=1) and Greenland (n=1). The main disease focus was diabetic retinopathy (n=30, 45%), followed by 'all eye care' (n=16, 24%). Most studies focused on targeted interventions to increase availability of services. Fewer than one-third of studies reported involving Indigenous communities when designing the service. 41 studies reflected on whether the model improved access, but none undertook rigorous evaluation or quantitative assessment.
The geographical and clinical scope of service delivery models to improve access to eye care for Indigenous peoples in high-income countries is narrow, with most studies focused on Australia and services for diabetic retinopathy. More and better engagement with Indigenous communities is required to design and implement accessible eye care services.
在全球范围内,有大约 3.7 亿土著人民。与非土著人民相比,土著人民的健康状况通常更差,包括更高的可避免视力损害率。造成这种眼科健康差距的大部分原因是阻碍他们获得眼科保健服务的障碍。我们进行了一项范围界定审查,以确定和总结旨在改善高收入国家土著人民获得眼科保健服务的交付模式。
2019 年 1 月在 MEDLINE、Embase 和全球卫生数据库中进行了检索,并于 2020 年 7 月进行了更新。如果研究描述了旨在针对土著人口(土著人口超过 50%)的眼科保健服务交付模式,则所有研究设计均符合条件。两名评审员独立筛选标题、摘要和全文文章,并完成数据图表。我们提取了有关出版物详细信息、研究背景、服务交付干预措施、结果和评估、与土著人民的互动以及针对的获取维度的数据。我们根据主题分析对发现进行了描述性总结。
我们筛选了 2604 篇摘要,有 67 篇研究符合我们的纳入标准。研究集中在澳大利亚(n=45)、美国(n=11)、加拿大(n=7)、新西兰(n=2)、中国台湾(n=1)和格陵兰(n=1)的土著人民。主要疾病重点是糖尿病视网膜病变(n=30,45%),其次是“所有眼科保健”(n=16,24%)。大多数研究侧重于增加服务可用性的针对性干预措施。只有不到三分之一的研究报告在设计服务时涉及土著社区。41 项研究反映了该模式是否改善了获取服务的机会,但没有一项进行严格的评估或定量评估。
改善高收入国家土著人民获得眼科保健服务的交付模式的地理和临床范围狭窄,大多数研究集中在澳大利亚和糖尿病视网膜病变服务上。需要更多和更好地与土著社区接触,以设计和实施可及的眼科保健服务。