Kuraparthy Sambasivaiah, Reddy Kumaraswamy M, Yadagiri Lakshmi Amancharla, Yutla Mutheeswaraiah, Venkata Phanindra Bobbidi, Kadainti Sarma V S, Reddy Ramasubba P V
Department of Medical oncology, Sri Venkateswara institute of Medical Sciences, Tirupati, India.
World J Surg Oncol. 2007 May 23;5:56. doi: 10.1186/1477-7819-5-56.
Breast cancer incidence in India is on rise. We report epidemiological, clinical and survival patterns of breast cancer patients from community perspective.
All breast cancer patients treated at this hospital from July 2000 to July 2005 were included. All had cytological or histological confirmation of breast cancer. TNM guidelines for staging and Immunohistochemistry to assess the receptor status were used. Either lumpectomy with axillary lymph node dissection or Modified radical mastectomy (MRM) was done for operable breast cancer, followed by 6 cycles of adjuvant chemotherapy with FAC or CMF regimens to patients with pT >1 cm or lymph node positive or estrogen receptor negative and radiotherapy to patients after breast conservation surgery, pT size > 5 cm, 4 or more positive nodes and stage IIIB disease. Patients with positive Estrogen receptor or Progesterone receptor were advised Tamoxifene 20 mg per day for 3 years. Descriptive analysis was performed. Independent T test and Chi-square test were used. Overall survival time was computed by Kaplan - Meier method.
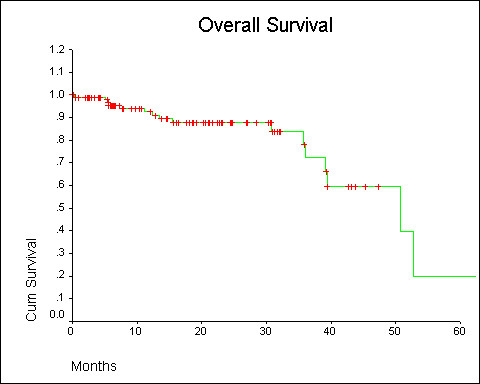
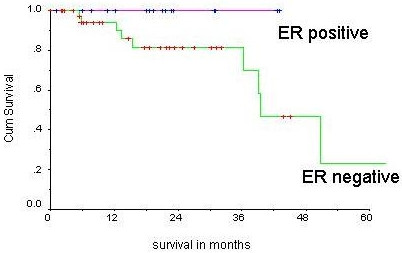
Of 1488 cancer patients, 122 (8.2%) had breast cancer. Of 122 patients, 96.7% had invasive breast carcinoma and 3.3% had sarcoma. 94% came from the rural and semi urban areas. Premenopausal women were 27%. The median age was 50 years. Stage I-6.8%, II-45.8%, III-22%, IV-6.8%, Bilateral breast cancer - 2.5%. The mean pT size was 3.9 cm. ER and PR were positive in 31.6% and 28.1% respectively. MRM was done in 93.8%, while 6.3% patients underwent breast conservation surgery. The mean of the lymph nodes dissected were 3. CMF and FAC regimens were used in 48.8% and 51.2% of patients respectively. FAC group were younger than the CMF group (43.6 yr vs. 54 yrs, P = 0.000). Toxicities were more in FAC than CMF group, alopecia (100% vs. 26.2%), grade2 or more emesis (31.8% vs. 9.2%), grade2 or more fatigue (40.9% vs.19%), anemia (43.1% vs. 16.6%). Median Survival for the cohort was 50.8 months. ER positive patients had better median survival (P = 0.05).
MRM was the most frequent surgical option. CMF and FAC showed equivalent survival. FAC chemotherapy was more toxic than CMF. ER positive tumors have superior survival. Overall 3 year survival was 70 percent.
印度乳腺癌发病率呈上升趋势。我们从社区角度报告乳腺癌患者的流行病学、临床及生存模式。
纳入2000年7月至2005年7月在本院接受治疗的所有乳腺癌患者。所有患者均经细胞学或组织学确诊为乳腺癌。采用TNM分期指南及免疫组织化学评估受体状态。对于可手术乳腺癌,行保乳手术加腋窝淋巴结清扫或改良根治性乳房切除术(MRM),对于pT>1 cm或淋巴结阳性或雌激素受体阴性的患者,术后给予6周期FAC或CMF方案辅助化疗,对于保乳手术后、pT大小>5 cm、4个或更多阳性淋巴结及IIIB期疾病的患者给予放疗。雌激素受体或孕激素受体阳性的患者,建议每天服用20 mg他莫昔芬,持续3年。进行描述性分析。采用独立t检验和卡方检验。采用Kaplan - Meier法计算总生存时间。
在1488例癌症患者中,122例(8.2%)患有乳腺癌。122例患者中,96.7%为浸润性乳腺癌,3.3%为肉瘤。94%来自农村和半城市地区。绝经前女性占27%。中位年龄为50岁。I期-6.8%,II期-45.8%,III期-22%,IV期-6.8%,双侧乳腺癌-2.5%。平均pT大小为3.9 cm。ER和PR阳性率分别为31.6%和28.1%。93.8%的患者行MRM,而6.3%的患者接受保乳手术。平均清扫淋巴结数为3个。48.8%和51.2%的患者分别使用CMF和FAC方案。FAC组患者比CMF组年轻(43.6岁对54岁,P = 0.000)。FAC组的毒性反应比CMF组更多,脱发(100%对26.2%),2级或更严重呕吐(31.8%对9.2%),2级或更严重疲劳(40.9%对19%),贫血(43.1%对16.6%)。该队列的中位生存期为50.8个月。ER阳性患者的中位生存期更好(P = 0.05)。
MRM是最常用的手术方式。CMF和FAC显示出相当的生存率。FAC化疗比CMF毒性更大。ER阳性肿瘤的生存率更高。总体3年生存率为70%。