Moore R Andrew, Derry Sheena, McQuay Henry J
Pain Research and Nuffield Department of Anaesthetics, University of Oxford, The Churchill, Headington, Oxford, UK.
BMC Musculoskelet Disord. 2007 Aug 3;8:73. doi: 10.1186/1471-2474-8-73.
Differences between gastrointestinal and cardiovascular effects of traditional NSAID or cyclooxygenase-2 selective inhibitor (coxib) are affected by drug, dose, duration, outcome definition, and patient gastrointestinal and cardiovascular risk factors. We calculated the absolute risk for each effect.
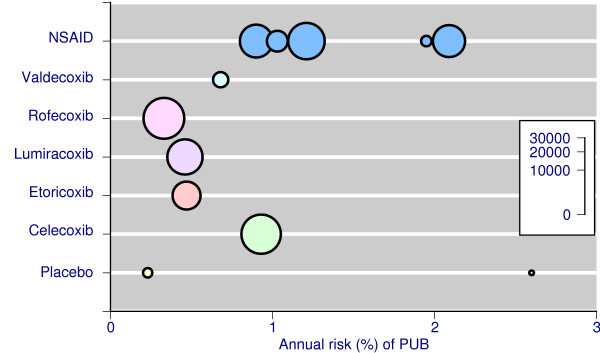
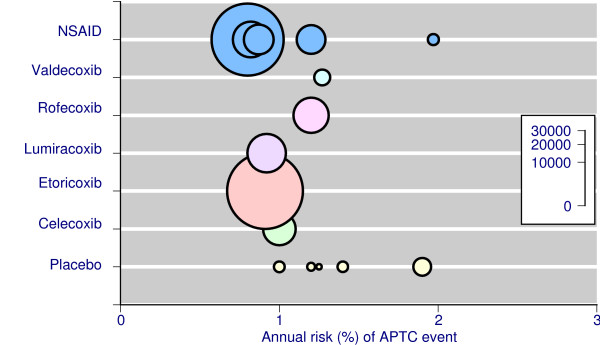
We sought studies with large amounts of information to calculate annualised rates for clearly defined gastrointestinal (complicated upper gastrointestinal perforations, ulcers, or bleeds, but not symptomatic or endoscopic ulcers) and serious cardiovascular outcomes (antiplatelet trial collaborators - APTC - outcome of fatal or nonfatal myocardial infarction or stroke, or vascular death).
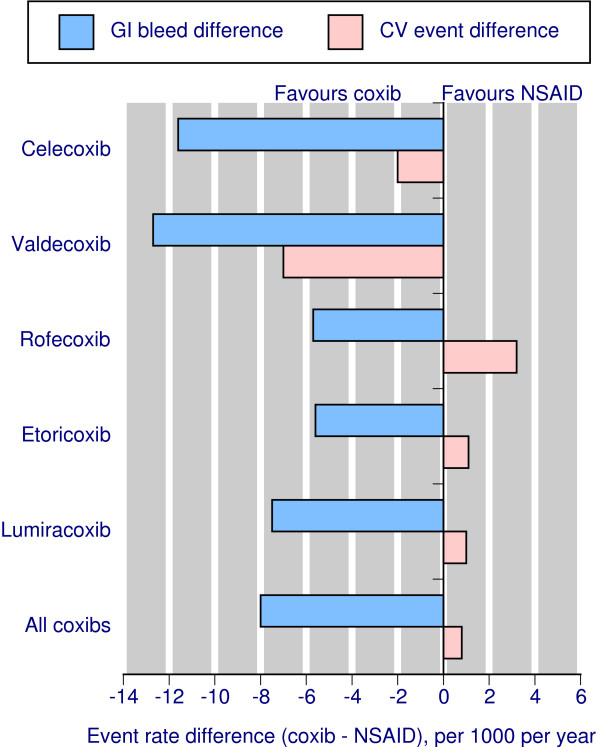
Meta-analyses and large randomised trials specifically analysing serious gastrointestinal bleeding or cardiovascular events occurring with five different coxibs had appropriate data. In total there were 439 complicated upper gastrointestinal events in 49,006 patient years of exposure and 948 serious cardiovascular events in 99,400 patient years of exposure. Complicated gastrointestinal events occurred less frequently with coxibs than NSAIDs; serious cardiovascular events occurred at approximately equal rates. For each coxib, the reduction in complicated upper gastrointestinal events was numerically greater than any increase in APTC events. In the overall comparison, for every 1000 patients treated for a year with coxib rather than NSAID, there would be eight fewer complicated upper gastrointestinal events, but one more fatal or nonfatal heart attack or stroke. Three coxib-NSAID comparisons had sufficient numbers of events for individual comparisons. For every 1000 patients treated for a year with celecoxib rather than an NSAID there would be 12 fewer upper gastrointestinal complications, and two fewer fatal or nonfatal heart attacks or strokes. For rofecoxib there would be six fewer upper gastrointestinal complications, but three more fatal or nonfatal heart attacks or strokes. For lumiracoxib there would be eight fewer upper gastrointestinal complications, but one more fatal or nonfatal heart attack or stroke.
Calculating annualised event rates for gastrointestinal and cardiovascular harm shows that while complicated gastrointestinal events occur more frequently with NSAIDs than coxibs, serious cardiovascular events occur at approximately equal rates. For each coxib, the reduction in complicated upper gastrointestinal events was numerically greater than any increase in APTC events.
传统非甾体抗炎药(NSAID)或环氧化酶-2选择性抑制剂(coxib)在胃肠道和心血管方面的作用差异受药物、剂量、疗程、结局定义以及患者胃肠道和心血管危险因素的影响。我们计算了每种作用的绝对风险。
我们寻找包含大量信息的研究,以计算明确界定的胃肠道(复杂性上消化道穿孔、溃疡或出血,但不包括有症状或内镜下溃疡)和严重心血管结局(抗血小板试验协作组 - APTC - 致命或非致命心肌梗死或中风,或血管性死亡的结局)的年化发生率。
对五种不同coxib发生的严重胃肠道出血或心血管事件进行专门分析的荟萃分析和大型随机试验有合适的数据。在总共49006患者年的暴露中,有439例复杂性上消化道事件,在99400患者年的暴露中有948例严重心血管事件。与NSAID相比,coxib导致的复杂性胃肠道事件发生频率更低;严重心血管事件的发生率大致相当。对于每种coxib,复杂性上消化道事件的减少在数值上大于APTC事件的任何增加。在总体比较中,每1000例接受coxib而非NSAID治疗一年的患者,复杂性上消化道事件会减少8例,但致命或非致命心脏病发作或中风会增加1例。三项coxib-NSAID比较有足够数量的事件进行个体比较。每1000例接受塞来昔布而非NSAID治疗一年的患者,上消化道并发症会减少12例,致命或非致命心脏病发作或中风会减少2例。对于罗非昔布,上消化道并发症会减少6例,但致命或非致命心脏病发作或中风会增加3例。对于鲁米昔布,上消化道并发症会减少8例,但致命或非致命心脏病发作或中风会增加1例。
计算胃肠道和心血管损害的年化事件发生率表明,虽然NSAID导致的复杂性胃肠道事件比coxib更频繁,但严重心血管事件的发生率大致相当。对于每种coxib,复杂性上消化道事件的减少在数值上大于APTC事件的任何增加。