Kasolo F C, Spinks J, Bima H, Bates M, Gompels U A
Virology Department, University Teaching Hospital, University of Zambia Medical School, Lusaka, Zambia.
J Med Virol. 2007 Oct;79(10):1555-61. doi: 10.1002/jmv.20952.
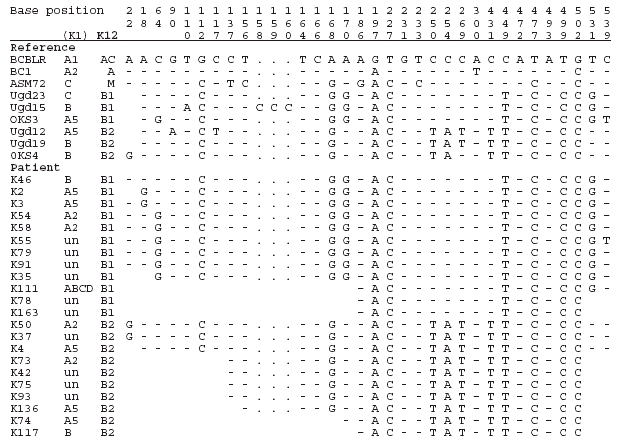
Kaposi's sarcoma-associated herpesvirus (KSHV or HHV-8) has been associated with several neoplasias, including childhood endemic Kaposi's sarcoma (KS). It is possible that strain genotypes could contribute to the differences in regional presentation (mainly sub-Saharan Africa), childhood infection, lack of male sex bias, distinct disseminated forms and rapid fatality observed for childhood endemic KS. Early studies, at the advent of the HIV/AIDS epidemic, identified only the K1-A5 genotype in childhood KS biopsies as well as blood of a few HIV positive and negative febrile infants in Zambia, a highly endemic region. This current enlarged study analyses blood infections of 200 hospitalized infants (6-34 months age) with symptoms of fever as well as upper respiratory tract infection, diarrhoea, rash or rhinitis. KSHV and HIV viraemia and were prevalent in this group, 22% and 39%, respectively. Multiple markers at both variable ends of the genome (K1, K12, and K14.1/K15) were examined, showing diverse previously adult-linked genotypes (K1 A2, A5, B, C3, D, with K12 B1 and B2 plus K14.1/K15 P or M) detected in both HIV positive and negative infants, demonstrating little restriction on KSHV genotypes for infant/childhood transmission in a childhood endemic KS endemic region. This supports the interpretation that the acquisition of childhood KSHV infections and subsequent development of KS are due to additional co-factors.
卡波西肉瘤相关疱疹病毒(KSHV 或 HHV - 8)与多种肿瘤形成有关,包括儿童地方性卡波西肉瘤(KS)。毒株基因型可能导致了在区域表现(主要是撒哈拉以南非洲地区)、儿童感染、不存在男性性别偏向、独特的播散形式以及儿童地方性 KS 所观察到的快速致死率等方面的差异。在 HIV/AIDS 流行初期的早期研究中,仅在儿童 KS 活检样本以及赞比亚(一个高流行地区)少数 HIV 阳性和阴性发热婴儿的血液中鉴定出 K1 - A5 基因型。当前这项扩大的研究分析了 200 名住院婴儿(6 - 34 个月大)的血液感染情况,这些婴儿有发热以及上呼吸道感染、腹泻、皮疹或鼻炎等症状。KSHV 和 HIV 病毒血症在该组中普遍存在,分别为 22%和 39%。对基因组两个可变末端的多个标记(K1、K12 和 K14.1/K15)进行了检测,结果显示在 HIV 阳性和阴性婴儿中均检测到多种先前与成人相关的基因型(K1 A2、A5、B、C3、D,K12 B1 和 B2 以及 K14.1/K15 P 或 M),这表明在儿童地方性 KS 流行地区,KSHV 基因型对婴儿/儿童传播几乎没有限制。这支持了以下解释,即儿童 KSHV 感染的获得以及随后 KS 的发展是由于其他共同因素。