Hurst Samia A, Forde Reidun, Reiter-Theil Stella, Slowther Anne-Marie, Perrier Arnaud, Pegoraro Renzo, Danis Marion
Institute for Biomedical Ethics, Geneva University Medical School, Switzerland.
BMC Health Serv Res. 2007 Aug 31;7:137. doi: 10.1186/1472-6963-7-137.
In response to limited resources, health care systems have adopted diverse cost-containment strategies and give priority to differing types of interventions. The perception of physicians, who witness the effects of these strategies, may provide useful insights regarding the impact of system-wide priority setting on access to care.
We conducted a cross-sectional survey to ascertain generalist physicians' perspectives on resources allocation and its consequences in Norway, Switzerland, Italy and the UK.
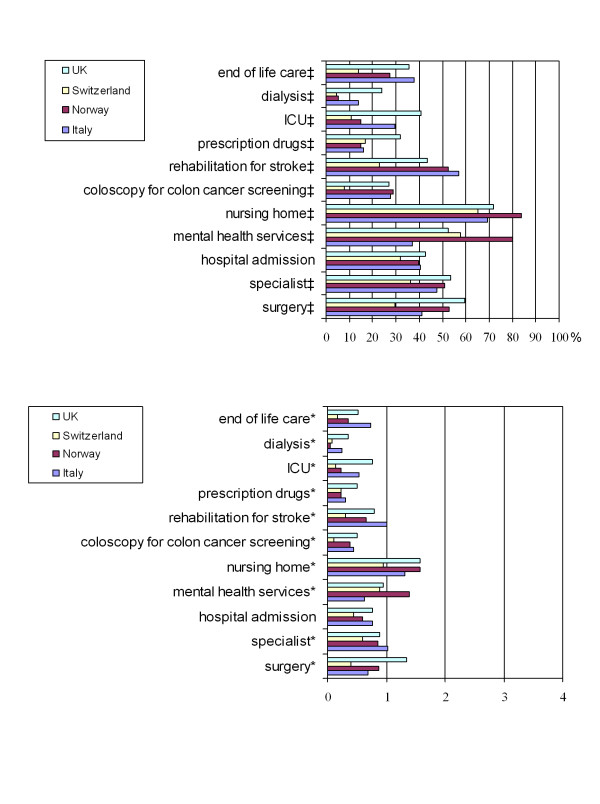
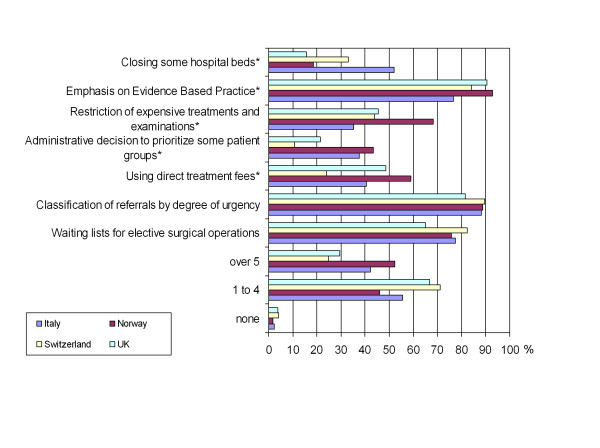
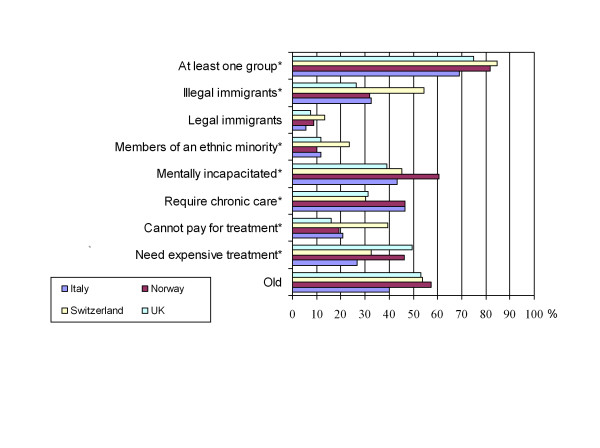
Survey respondents (N = 656, response rate 43%) ranged in age from 28-82, and averaged 25 years in practice. Most respondents (87.7%) perceived some resources as scarce, with the most restrictive being: access to nursing home, mental health services, referral to a specialist, and rehabilitation for stroke. Respondents attributed adverse outcomes to scarcity, and some respondents had encountered severe adverse events such as death or permanent disability. Despite universal coverage, 45.6% of respondents reported instances of underinsurance. Most respondents (78.7%) also reported some patient groups as more likely than others to be denied beneficial care on the basis of cost. Almost all respondents (97.3%) found at least one cost-containment policy acceptable. The types of policies preferred suggest that respondents are willing to participate in cost-containment, and do not want to be guided by administrative rules (11.2%) or restrictions on hospital beds (10.7%).
Physician reports can provide an indication of how organizational factors may affect availability and equity of health care services. Physicians are willing to participate in cost-containment decisions, rather than be guided by administrative rules. Tools should be developed to enable physicians, who are in a unique position to observe unequal access or discrimination in their health care environment, to address these issues in a more targeted way.
为应对资源有限的情况,医疗保健系统采取了多种成本控制策略,并优先考虑不同类型的干预措施。见证这些策略效果的医生的看法,可能会为全系统的优先事项设定对医疗服务可及性的影响提供有用的见解。
我们进行了一项横断面调查,以确定挪威、瑞士、意大利和英国的全科医生对资源分配及其后果的看法。
调查受访者(N = 656,回复率43%)年龄在28至82岁之间,平均执业年限为25年。大多数受访者(87.7%)认为某些资源稀缺,其中限制最大的是:养老院服务、心理健康服务、转诊至专科医生以及中风康复服务。受访者将不良后果归因于资源稀缺,一些受访者还遭遇过严重的不良事件,如死亡或永久性残疾。尽管有全民医保,但45.6%的受访者报告了保险不足的情况。大多数受访者(78.7%)还报告说,某些患者群体比其他群体更有可能因成本原因而被拒绝接受有益的治疗。几乎所有受访者(97.3%)都认为至少有一种成本控制政策是可以接受的。他们偏好的政策类型表明,受访者愿意参与成本控制,并且不希望受到行政规定(11.2%)或医院床位限制(10.7%)的指导。
医生的报告可以表明组织因素可能如何影响医疗服务的可及性和公平性。医生愿意参与成本控制决策,而不是受行政规定的指导。应开发工具,使处于独特地位、能够观察到其医疗环境中存在的不平等可及性或歧视现象的医生,能够更有针对性地解决这些问题。