Bell David J, Nyirongo Suzgo K, Mukaka Mavuto, Zijlstra Ed E, Plowe Christopher V, Molyneux Malcolm E, Ward Steve A, Winstanley Peter A
Department of Molecular and Biochemical Parasitology, Liverpool School of Tropical Medicine, Liverpool, United Kingdom.
PLoS One. 2008 Feb 13;3(2):e1578. doi: 10.1371/journal.pone.0001578.
In Malawi, there has been a return of Plasmodium falciparum sensitivity to chloroquine (CQ) since sulfadoxine-pyrimethamine (SP) replaced CQ as first line treatment for uncomplicated malaria. When used for prophylaxis, Amodiaquine (AQ) was associated with agranulocytosis but is considered safe for treatment and is increasingly being used in Africa. Here we compare the efficacy, safety and selection of resistance using SP or CQ+SP or artesunate (ART)+SP or AQ+SP for the treatment of uncomplicated falciparum malaria.
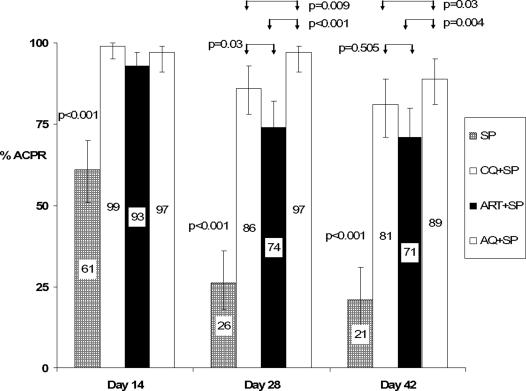
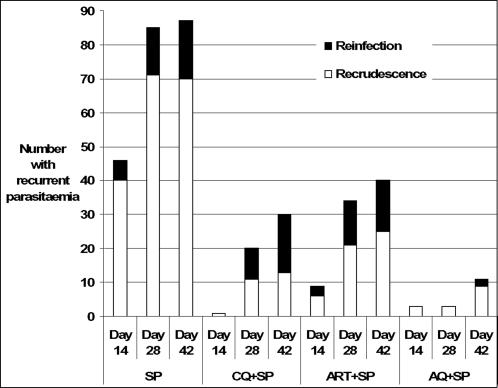
455 children aged 1-5 years were recruited into a double-blinded randomised trial comparing SP to the three combination therapies. Using intention to treat analysis with missing outcomes treated as successes, and without adjustment to distinguish recrudescence from new infections, the day 28 adequate clinical and parasitological response (ACPR) rate for SP was 25%, inferior to each of the three combination therapies (p<0.001). AQ+SP had an ACPR rate of 97%, higher than CQ+SP (81%) and ART+SP (70%), p<0.001. Nineteen children developed a neutropenia of </=0.5x10(3) cells/microl by day 14, more commonly after AQ+SP (p = 0.03). The mutation pfcrt 76T, associated with CQ resistance, was detected in none of the pre-treatment or post-treatment parasites. The prevalence of the pfmdr1 86Y mutation was higher after treatment with AQ+SP than after SP, p = 0.002.
The combination AQ+SP was highly efficacious, despite the low efficacy of SP alone; however, we found evidence that AQ may exert selective pressure for resistance associated mutations many weeks after treatment. This study confirms the return of CQ sensitivity in Malawi and importantly, shows no evidence of the re-emergence of pfcrt 76T after treatment with CQ or AQ. Given the safety record of AQ when used as a prophylaxis, our observations of marked falls in neutrophil counts in the AQ+SP group requires further scrutiny.
Controlled-Trials.com ISRCTN22075368.
在马拉维,自从磺胺多辛-乙胺嘧啶(SP)取代氯喹(CQ)成为单纯性疟疾的一线治疗药物后,恶性疟原虫对氯喹(CQ)的敏感性又恢复了。阿莫地喹(AQ)用于预防时与粒细胞缺乏症有关,但被认为用于治疗是安全的,并且在非洲越来越多地被使用。在此,我们比较使用SP或CQ + SP或青蒿琥酯(ART)+ SP或AQ + SP治疗单纯性恶性疟疾的疗效、安全性及耐药性选择情况。
455名1至5岁儿童被纳入一项双盲随机试验,比较SP与三种联合疗法。采用意向性分析,将缺失结局视为成功,且不进行区分复发与新感染的调整,SP在第28天的充分临床和寄生虫学反应(ACPR)率为25%,低于三种联合疗法中的任何一种(p < 0.001)。AQ + SP的ACPR率为97%,高于CQ + SP(81%)和ART + SP(70%),p < 0.001。到第14天,19名儿童出现了中性粒细胞减少至≤0.5×10³个/微升,在AQ + SP治疗后更为常见(p = 0.03)。在治疗前和治疗后的寄生虫中均未检测到与CQ耐药相关的pfcrt 76T突变。与SP治疗后相比,AQ + SP治疗后pfmdr1 86Y突变的发生率更高,p = 0.002。
尽管单独使用SP疗效较低,但AQ + SP联合疗法非常有效;然而,我们发现有证据表明,AQ可能在治疗后数周对耐药相关突变施加选择性压力。本研究证实了马拉维恶性疟原虫对CQ敏感性的恢复,重要的是,未显示在用CQ或AQ治疗后pfcrt 76T再次出现的证据。鉴于AQ用作预防药物时的安全记录,我们在AQ + SP组中观察到的中性粒细胞计数显著下降需要进一步审查。
Controlled-Trials.com ISRCTN22075368 。