Novartis Institute for Tropical Diseases, Singapore.
PLoS Negl Trop Dis. 2008 Mar 12;2(3):e196. doi: 10.1371/journal.pntd.0000196.
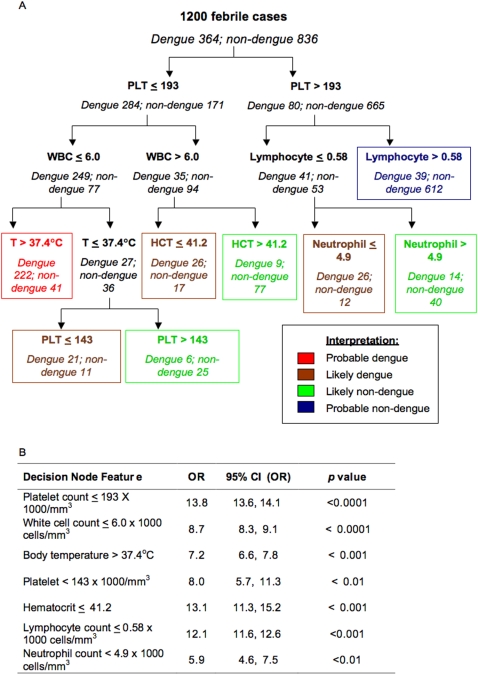
Dengue is re-emerging throughout the tropical world, causing frequent recurrent epidemics. The initial clinical manifestation of dengue often is confused with other febrile states confounding both clinical management and disease surveillance. Evidence-based triage strategies that identify individuals likely to be in the early stages of dengue illness can direct patient stratification for clinical investigations, management, and virological surveillance. Here we report the identification of algorithms that differentiate dengue from other febrile illnesses in the primary care setting and predict severe disease in adults.
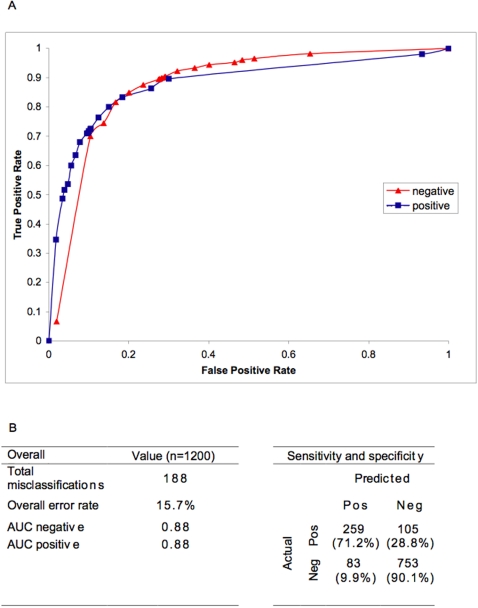
A total of 1,200 patients presenting in the first 72 hours of acute febrile illness were recruited and followed up for up to a 4-week period prospectively; 1,012 of these were recruited from Singapore and 188 from Vietnam. Of these, 364 were dengue RT-PCR positive; 173 had dengue fever, 171 had dengue hemorrhagic fever, and 20 had dengue shock syndrome as final diagnosis. Using a C4.5 decision tree classifier for analysis of all clinical, haematological, and virological data, we obtained a diagnostic algorithm that differentiates dengue from non-dengue febrile illness with an accuracy of 84.7%. The algorithm can be used differently in different disease prevalence to yield clinically useful positive and negative predictive values. Furthermore, an algorithm using platelet count, crossover threshold value of a real-time RT-PCR for dengue viral RNA, and presence of pre-existing anti-dengue IgG antibodies in sequential order identified cases with sensitivity and specificity of 78.2% and 80.2%, respectively, that eventually developed thrombocytopenia of 50,000 platelet/mm(3) or less, a level previously shown to be associated with haemorrhage and shock in adults with dengue fever.
This study shows a proof-of-concept that decision algorithms using simple clinical and haematological parameters can predict diagnosis and prognosis of dengue disease, a finding that could prove useful in disease management and surveillance.
登革热正在热带地区重新出现,导致频繁的复发性流行。登革热的初始临床表现常与其他发热状态混淆,给临床管理和疾病监测带来困难。基于证据的分诊策略可以识别出可能处于登革热早期的个体,从而对患者进行分层,以便进行临床检查、管理和病毒学监测。在此,我们报告了在初级保健环境中区分登革热与其他发热性疾病并预测成人重症疾病的算法的鉴定。
共招募了 1200 例在急性发热病的前 72 小时内就诊的患者,并前瞻性随访 4 周;其中 1012 例来自新加坡,188 例来自越南。这些患者中,364 例登革热 RT-PCR 阳性;173 例为登革热,171 例为登革出血热,20 例为登革热休克综合征。使用 C4.5 决策树分类器对所有临床、血液学和病毒学数据进行分析,我们获得了一种可将登革热与非登革热发热病区分开的诊断算法,准确率为 84.7%。该算法可根据不同的疾病流行情况以不同的方式使用,从而产生具有临床意义的阳性和阴性预测值。此外,使用血小板计数、登革热病毒 RNA 的实时 RT-PCR 交叉阈值以及连续顺序存在的预先存在的抗登革热 IgG 抗体的算法,可以识别出敏感性和特异性分别为 78.2%和 80.2%的病例,这些病例最终会出现血小板计数为 50000/mm(3)或更低的血小板减少症,这一水平以前曾与成人登革热中的出血和休克相关。
本研究证明了一种概念验证,即使用简单的临床和血液学参数的决策算法可以预测登革热疾病的诊断和预后,这一发现可能对疾病管理和监测具有重要意义。