Gérardin Patrick, Barau Georges, Michault Alain, Bintner Marc, Randrianaivo Hanitra, Choker Ghassan, Lenglet Yann, Touret Yasmina, Bouveret Anne, Grivard Philippe, Le Roux Karin, Blanc Séverine, Schuffenecker Isabelle, Couderc Thérèse, Arenzana-Seisdedos Fernando, Lecuit Marc, Robillard Pierre-Yves
Neonatal and Pediatric Intensive Care Unit, Pôle Mère-Enfant, Groupe Hospitalier Sud-Réunion, Saint-Pierre, La Réunion, France.
PLoS Med. 2008 Mar 18;5(3):e60. doi: 10.1371/journal.pmed.0050060.
An outbreak of chikungunya virus affected over one-third of the population of La Réunion Island between March 2005 and December 2006. In June 2005, we identified the first case of mother-to-child chikungunya virus transmission at the Groupe Hospitalier Sud-Réunion level-3 maternity department. The goal of this prospective study was to characterize the epidemiological, clinical, biological, and radiological features and outcomes of all the cases of vertically transmitted chikungunya infections recorded at our institution during this outbreak.
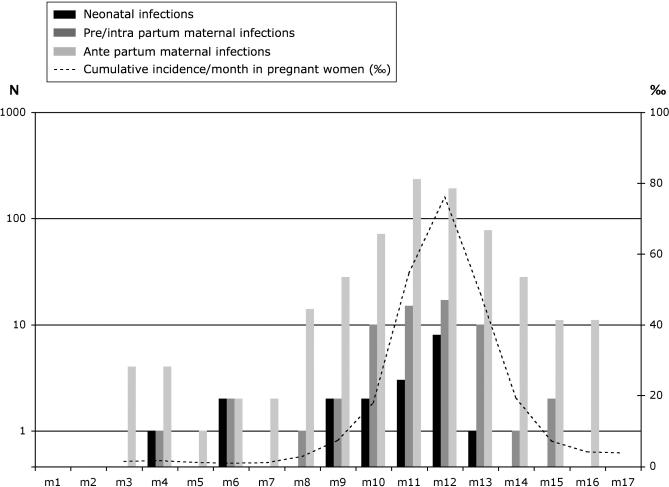
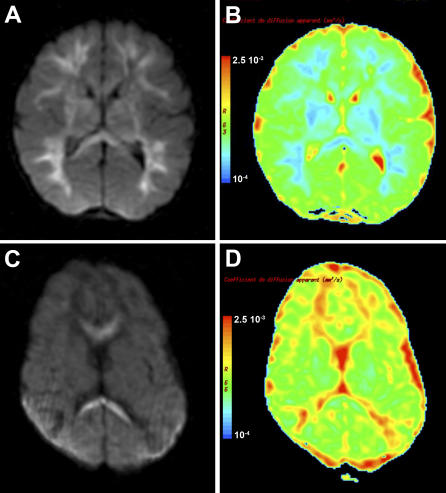
Over 22 mo, 7,504 women delivered 7,629 viable neonates; 678 (9.0%) of these parturient women were infected (positive RT-PCR or IgM serology) during antepartum, and 61 (0.8%) in pre- or intrapartum. With the exception of three early fetal deaths, vertical transmission was exclusively observed in near-term deliveries (median duration of gestation: 38 wk, range 35-40 wk) in the context of intrapartum viremia (19 cases of vertical transmission out of 39 women with intrapartum viremia, prevalence rate 0.25%, vertical transmission rate 48.7%). Cesarean section had no protective effect on transmission. All infected neonates were asymptomatic at birth, and median onset of neonatal disease was 4 d (range 3-7 d). Pain, prostration, and fever were present in 100% of cases and thrombocytopenia in 89%. Severe illness was observed in ten cases (52.6%) and mainly consisted of encephalopathy (n = 9; 90%). These nine children had pathologic MRI findings (brain swelling, n = 9; cerebral hemorrhages, n = 2), and four evolved towards persistent disabilities.
Mother-to-child chikungunya virus transmission is frequent in the context of intrapartum maternal viremia, and often leads to severe neonatal infection. Chikungunya represents a substantial risk for neonates born to viremic parturients that should be taken into account by clinicians and public health authorities in the event of a chikungunya outbreak.
2005年3月至2006年12月期间,留尼汪岛三分之一以上的人口受到基孔肯雅病毒疫情影响。2005年6月,我们在留尼汪岛南部集团医院三级产科部门确认了首例母婴基孔肯雅病毒传播病例。这项前瞻性研究的目的是描述在此次疫情期间我们机构记录的所有垂直传播的基孔肯雅病毒感染病例的流行病学、临床、生物学和放射学特征及结局。
在22个月的时间里,7504名妇女分娩了7629名存活新生儿;其中678名(9.0%)产妇在产前感染(逆转录聚合酶链反应阳性或IgM血清学阳性),61名(0.8%)在产前或产时感染。除3例早期胎儿死亡外,垂直传播仅在产时病毒血症情况下的近足月分娩中观察到(妊娠中位持续时间:38周,范围35 - 40周)(39例产时病毒血症的妇女中有19例垂直传播,患病率0.25%,垂直传播率48.7%)。剖宫产对传播没有保护作用。所有感染新生儿出生时均无症状,新生儿疾病的中位发病时间为4天(范围3 - 7天)。所有病例均有疼痛、虚脱和发热,89%有血小板减少。10例(52.6%)出现严重疾病,主要为脑病(9例;90%)。这9名儿童的MRI检查有病理表现(脑肿胀,9例;脑出血,2例),4例发展为持续性残疾。
在产时母亲病毒血症的情况下,母婴基孔肯雅病毒传播很常见,且常导致严重的新生儿感染。基孔肯雅病毒对病毒血症产妇所生新生儿构成重大风险,在基孔肯雅病毒疫情爆发时,临床医生和公共卫生当局应予以考虑。