Forestier Christiane, Guelon Dominique, Cluytens Valérie, Gillart Thierry, Sirot Jacques, De Champs Christophe
Université de Clermont 1 UFR Pharmacie Laboratoire de Bactériologie, 28 place Henri Dunant 63000 Clermont-Ferrand France.
Crit Care. 2008;12(3):R69. doi: 10.1186/cc6907. Epub 2008 May 20.
Preventing carriage of potentially pathogenic micro-organisms from the aerodigestive tract is an infection control strategy used to reduce the occurrence of ventilator-associated pneumonia in intensive care units. However, antibiotic use in selective decontamination protocols is controversial. The purpose of this study was to investigate the effect of oral administration of a probiotic, namely Lactobacillus, on gastric and respiratory tract colonization/infection with Pseudomonas aeruginosa strains. Our hypothesis was that an indigenous flora should exhibit a protective effect against secondary colonization.
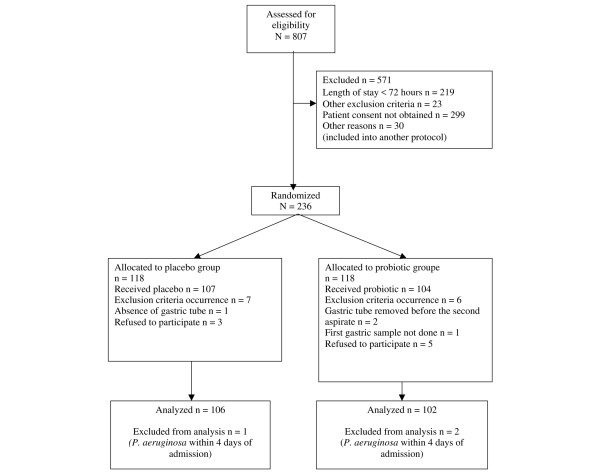
We conducted a prospective, randomized, double-blind, placebo-controlled pilot study between March 2003 and October 2004 in a 17-bed intensive care unit of a teaching hospital in Clermont-Ferrand, France. Consecutive patients with a unit stay of longer than 48 hours were included, 106 in the placebo group and 102 in the probiotic group. Through a nasogastric feeding tube, patients received either 109 colony-forming units unity forming colony of Lactobacillus casei rhamnosus or placebo twice daily, from the third day after admission to discharge. Digestive tract carriage of P. aeruginosa was monitored by cultures of gastric aspirates at admission, once a week thereafter and on discharge. In addition, bacteriological analyses of respiratory tract specimens were conducted to determine patient infectious status.
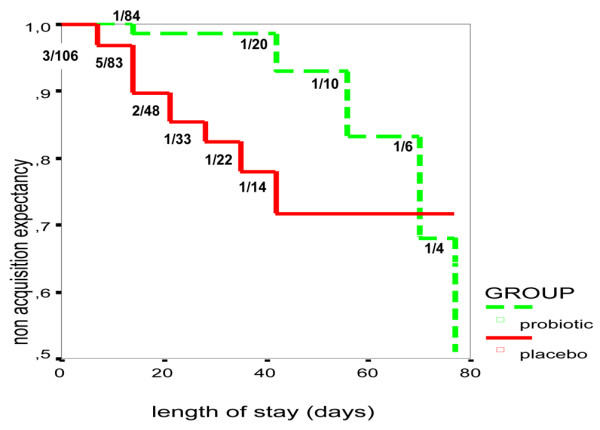
The occurrence of P. aeruginosa respiratory colonization and/or infection was significantly delayed in the probiotic group, with a difference in median delay to acquisition of 11 days versus 50 days (P = 0.01), and a nonacquisition expectancy mean of 69 days versus 77 days (P = 0.01). The occurrence of ventilator-associated pneumonia due to P. aeruginosa in the patients receiving the probiotic was less frequent, although not significantly reduced, in patients in the probiotic group (2.9%) compared with those in the placebo group (7.5%). After multivariate Cox proportional hazards modelling, the absence of probiotic treatment increased the risk for P. aeruginosa colonization in respiratory tract (adjusted hazard ratio = 3.2, 95% confidence interval - 1.1 to 9.1).
In this pilot study, oral administration of a probiotic delayed respiratory tract colonization/infection by P. aeruginosa.
The trial registration number for this study is NCT00604110.
防止潜在致病微生物在气消化道的定植是一种感染控制策略,用于减少重症监护病房呼吸机相关性肺炎的发生。然而,在选择性去污方案中使用抗生素存在争议。本研究的目的是调查口服益生菌(即乳酸杆菌)对铜绿假单胞菌菌株在胃和呼吸道的定植/感染的影响。我们的假设是,本土菌群应表现出对二次定植的保护作用。
2003年3月至2004年10月,我们在法国克莱蒙费朗一家教学医院的一个拥有17张床位的重症监护病房进行了一项前瞻性、随机、双盲、安慰剂对照的试点研究。纳入在该病房住院时间超过48小时的连续患者,安慰剂组106例,益生菌组102例。从入院第三天至出院,患者通过鼻胃饲管每天接受两次10⁹ 干酪乳杆菌鼠李糖亚种菌落形成单位或安慰剂。入院时通过胃吸出物培养监测铜绿假单胞菌在消化道的定植情况,此后每周一次,直至出院。此外,对呼吸道标本进行细菌学分析以确定患者的感染状态。
益生菌组铜绿假单胞菌呼吸道定植和/或感染的发生明显延迟,获得定植的中位延迟时间差异为11天对50天(P = 0.01),未获得定植的预期均值为69天对77天(P = 0.01)。接受益生菌治疗的患者中,由铜绿假单胞菌引起的呼吸机相关性肺炎的发生率较低,与安慰剂组(7.5%)相比,益生菌组患者中该发生率为2.9%,虽未显著降低。经过多变量Cox比例风险建模后,未进行益生菌治疗会增加呼吸道铜绿假单胞菌定植的风险(调整后的风险比 = 3.2,95%置信区间 - 1.1至9.1)。
在这项试点研究中,口服益生菌延迟了铜绿假单胞菌在呼吸道的定植/感染。
本研究的试验注册号为NCT00604110。