Head and Neck Service, Department of Surgery, Memorial Sloan-Kettering Cancer Center, 1275 York Avenue, New York, NY 10021, USA.
Oral Oncol. 2009 Apr-May;45(4-5):394-401. doi: 10.1016/j.oraloncology.2008.05.017. Epub 2008 Jul 31.
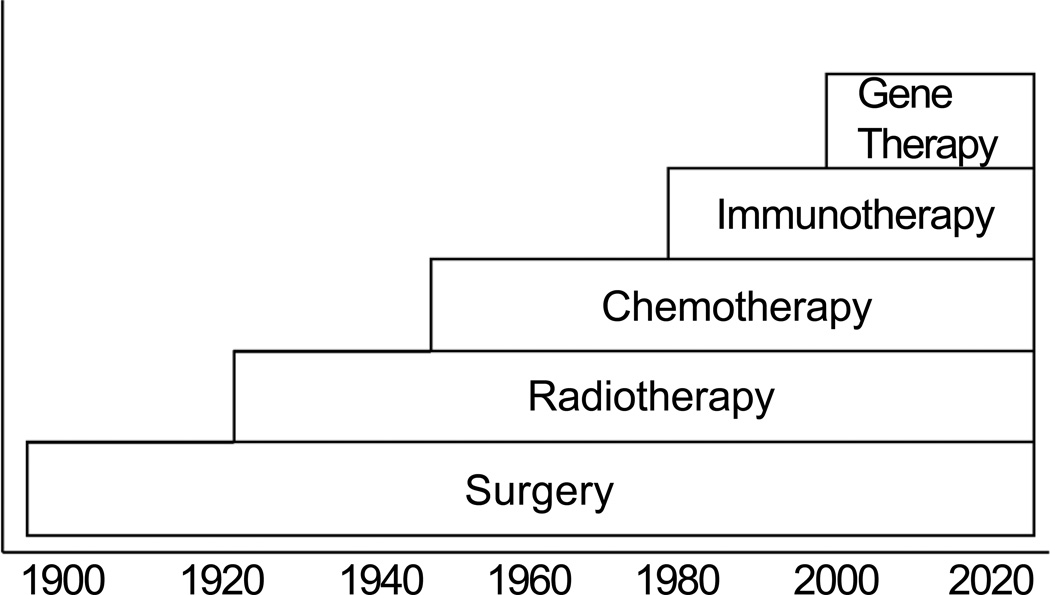
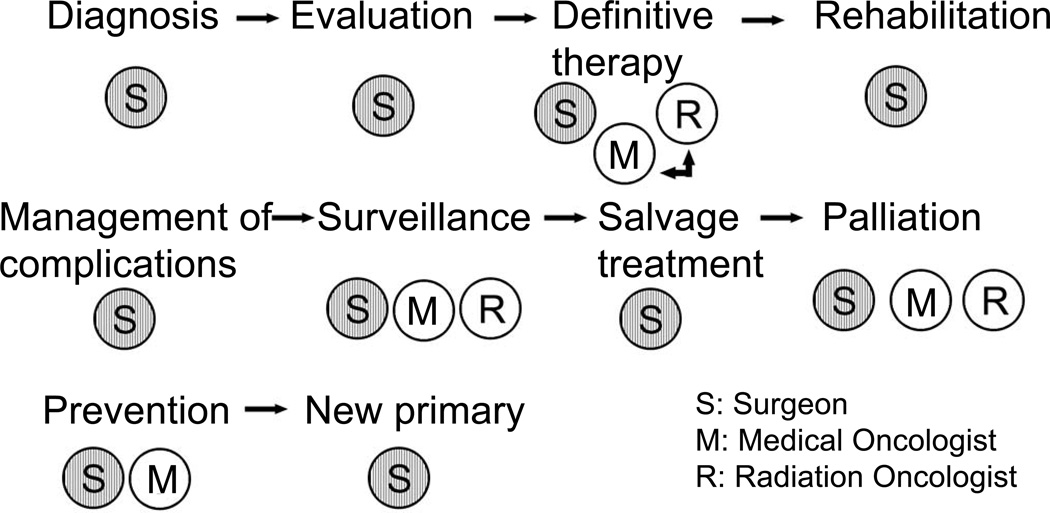
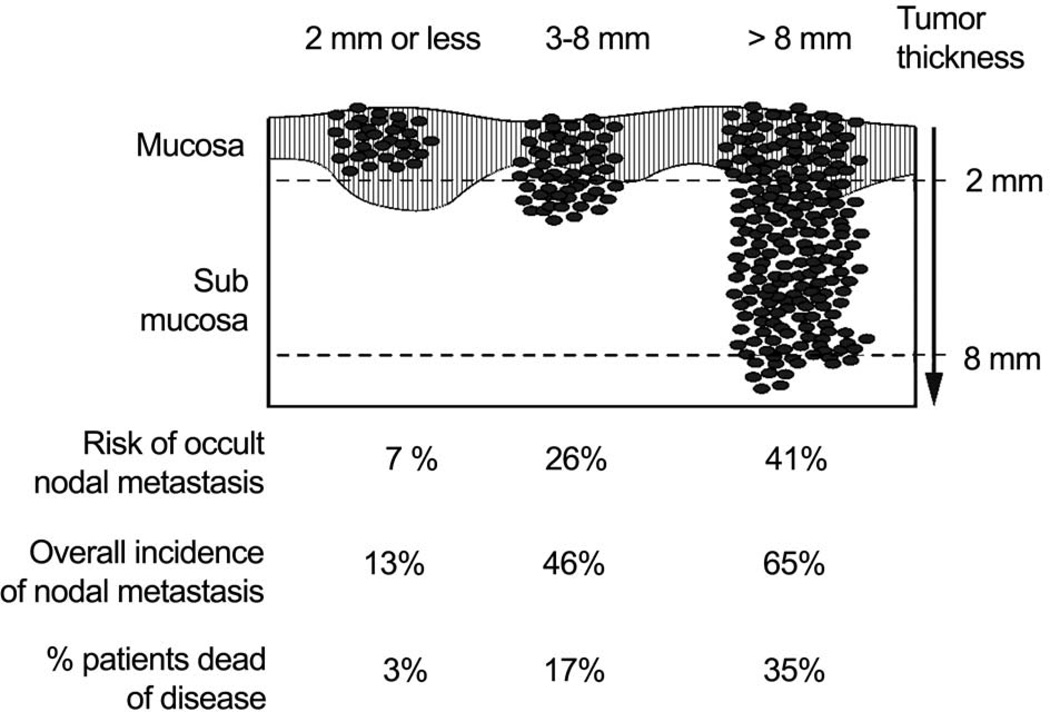
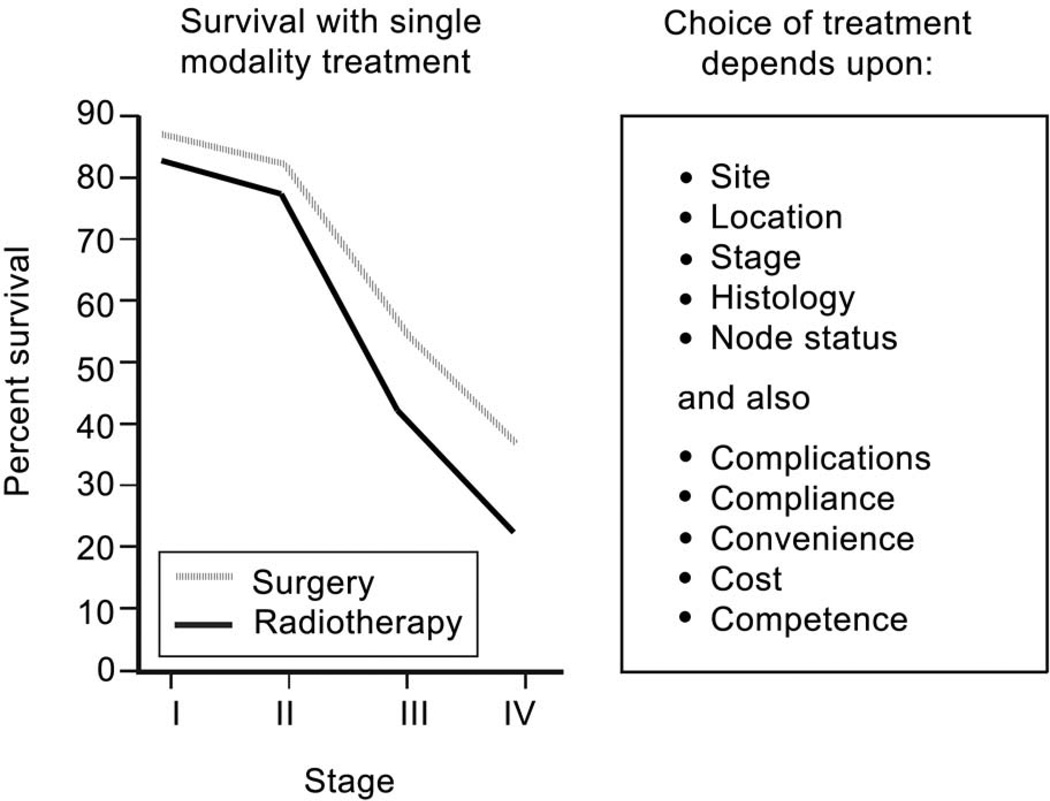
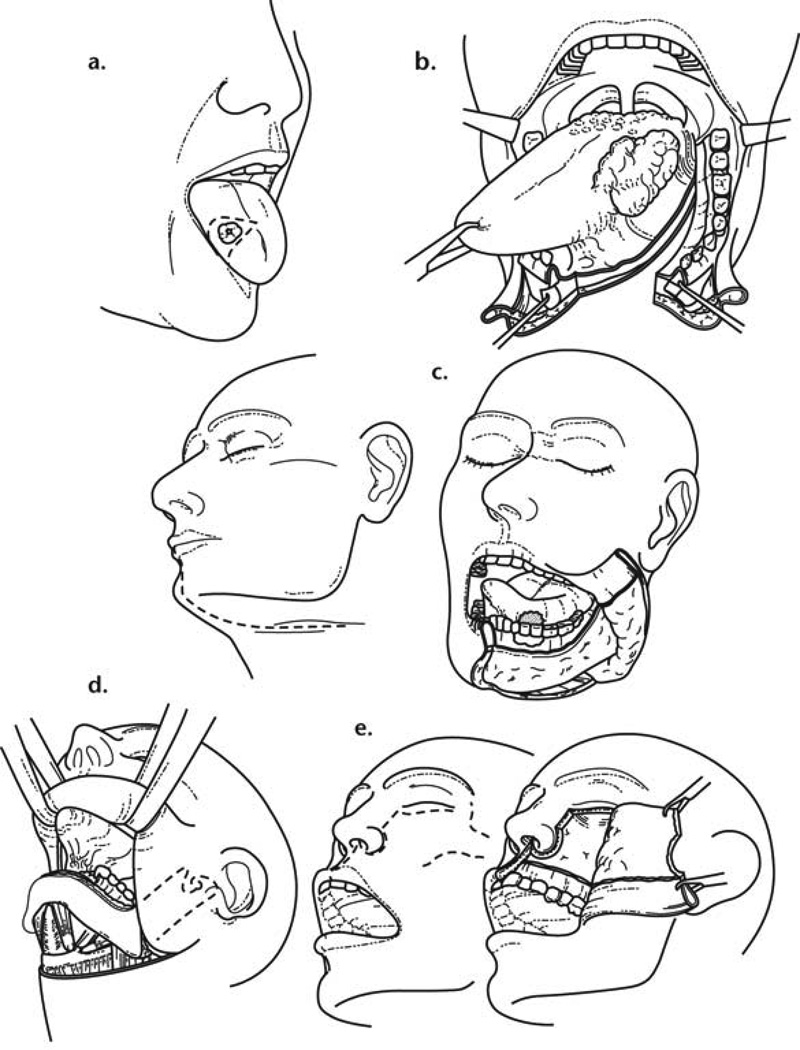
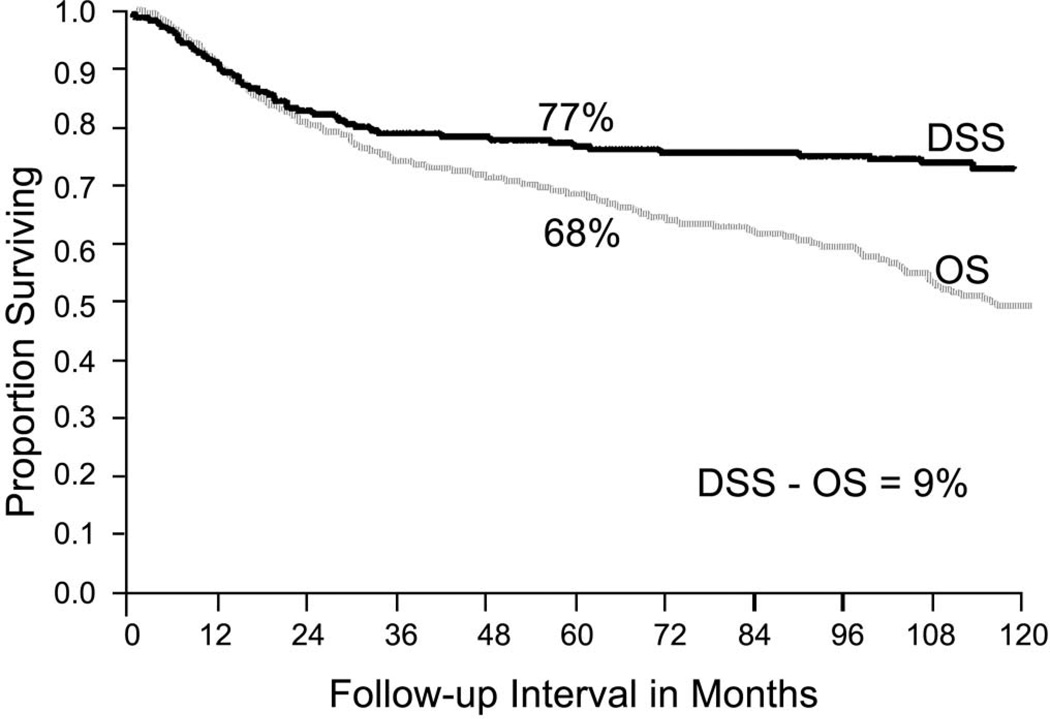
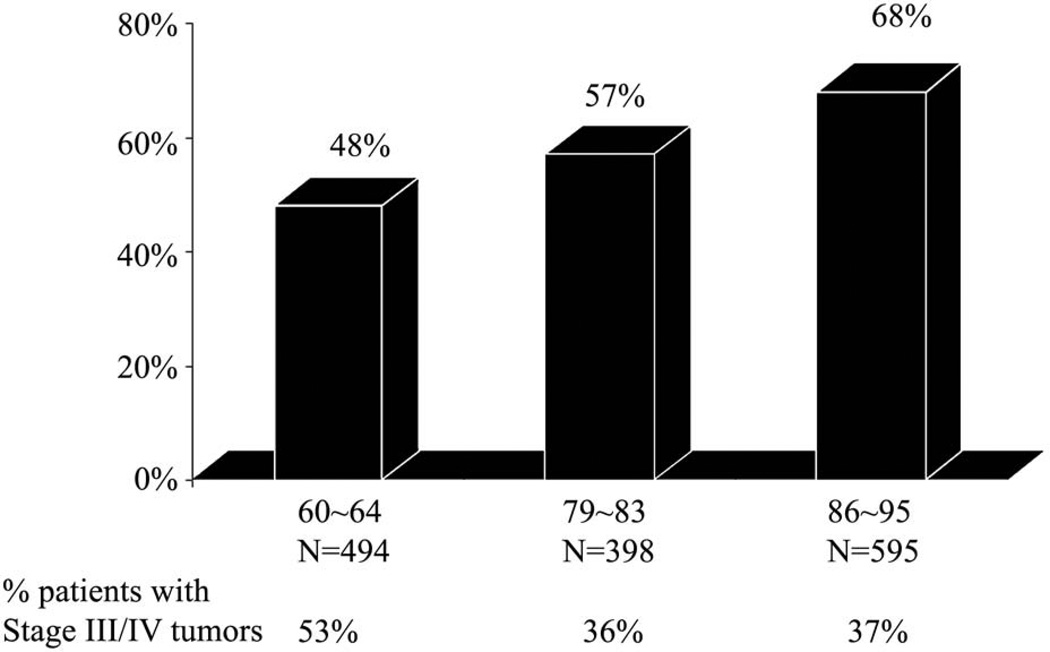
Oral cancer is the sixth most common cancer worldwide, with a high prevalence in South Asia. Tobacco and alcohol consumption remain the most dominant etiologic factors, however HPV has been recently implicated in oral cancer. Surgery is the most well established mode of initial definitive treatment for a majority of oral cancers. The factors that affect choice of treatment are related to the tumor and the patient. Primary site, location, size, proximity to bone, and depth of infiltration are factors which influence a particular surgical approach. Tumors that approach or involve the mandible require specific understanding of the mechanism of bone involvement. This facilitates the employment of mandible sparing approaches such as marginal mandibulectomy and mandibulotomy. Reconstruction of major surgical defects in the oral cavity requires use of a free flap. The radial forearm free flap provides excellent soft tissue and lining for soft tissue defects in the oral cavity. The fibula free flap remains the choice for mandibular reconstruction. Over the course of the past thirty years there has been improvement in the overall survival of patients with oral carcinoma largely due to the improved understanding of the biology of local progression, early identification and treatment of metastatic lymph nodes in the neck, and employment of adjuvant post-operative radiotherapy or chemoradiotherapy. The role of surgery in primary squamous cell carcinomas in other sites in the head and neck has evolved with integration of multidisciplinary treatment approaches employing chemotherapy and radiotherapy either sequentially or concurrently. Thus, larynx preservation with concurrent chemoradiotherapy has become the standard of care for locally advanced carcinomas of the larynx or pharynx requiring total laryngectomy. On the other hand, for early staged tumors of the larynx and pharynx, transoral laser microsurgery has become an effective means of local control of these lesions. Advances in skull base surgery have significantly improved the survivorship of patients with malignant tumors of the paranasal sinuses approaching or involving the skull base. Surgery thus remains the mainstay of management of a majority of neoplasms arising in the head and neck area. Similarly, the role of the surgeon is essential throughout the life history of a patient with a malignant neoplasm in the head and neck area, from initial diagnosis through definitive treatment, post-treatment surveillance, management of complications, rehabilitation of the sequelae of treatment, and finally for palliation of symptoms.
口腔癌是全球第六大常见癌症,在南亚地区较为普遍。吸烟和饮酒仍然是最主要的病因因素,但 HPV 最近也被认为与口腔癌有关。手术是治疗大多数口腔癌的最成熟的初始确定性治疗方法。影响治疗选择的因素与肿瘤和患者有关。原发部位、位置、大小、与骨骼的接近程度以及浸润深度是影响特定手术方法的因素。接近或涉及下颌骨的肿瘤需要对骨骼受累机制有特定的了解。这有助于采用下颌骨保留方法,如边缘下颌骨切除术和下颌骨切开术。口腔内大手术缺损的重建需要使用游离皮瓣。游离前臂皮瓣为口腔内软组织缺损提供了极好的软组织和衬里。游离腓骨皮瓣仍然是下颌骨重建的首选。在过去的三十年中,口腔癌患者的总体生存率有所提高,这主要是由于对局部进展生物学的认识的提高,对颈部转移性淋巴结的早期识别和治疗,以及辅助术后放疗或放化疗的应用。手术在头颈部其他部位原发性鳞状细胞癌中的作用随着多学科治疗方法的整合而发展,这些方法采用化疗和放疗顺序或同时应用。因此,喉保留伴同期放化疗已成为需要全喉切除术的局部晚期喉或咽癌的标准治疗方法。另一方面,对于早期喉和咽肿瘤,经口激光微创手术已成为局部控制这些病变的有效手段。颅底手术的进步显著提高了侵犯或涉及颅底的鼻窦恶性肿瘤患者的生存率。因此,手术仍然是治疗头颈部大多数肿瘤的主要方法。同样,外科医生在头颈部恶性肿瘤患者的整个病史中都发挥着重要作用,从最初的诊断到确定性治疗、治疗后监测、并发症的管理、治疗后遗症的康复,最后是缓解症状。